Exposing KRAS G12C: Not Your Usual Suspect in NSCLC
Emerging 1L Combination Strategies for KRAS G12C–mutant NSCLC
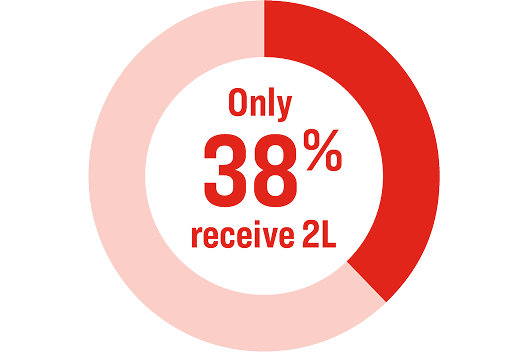
Clinical Gaps Remain: Of Patients Who Receive 1L, Only 38% Receive 2L Therapy Where Targeted Therapies are Approved Today1-3
Immunotherapy (IO) with or without chemotherapy is the standard of care (SOC) in KRAS G12C–mutant non-small cell lung cancer (NSCLC) with some exceptions. Programmed death-ligand 1 (PD-L1) levels are used to determine the appropriate first line (1L) systemic therapy.1,2 In the US, the most common 1L regimens include pembrolizumab (IO) alone or in combination with platinum-based chemotherapy3
- Non-squamous cell carcinoma, no history of smoking, PD-L1 ≥1% are associated with better outcomes
- Older age, performance status ≥1, brain metastasis at 1L, KEAP1 and STK11 co-mutations are associated with poorer outcomes
Recommendations that guide treatment-related decisions in KRAS G12C–mutant NSCLC are typically based on consideration for at least some these prognostic factors. Patient preference is also generally considered to ensure that there is shared treatment decision making.4
- As PD-L1≥1% is also a predictor for better outcomes, it could provide a rationale in part for the prolonged survival (median OS = 30.2 months) seen in patients treated with IO alone when compared to patients treated with combination or chemotherapy alone (median OS = 10.2 months and 9.2 months, respectively)5
- OS in second line (2L) was comparable irrespective of the treatment regimen used:5
- IO alone = 11.3 months
- Chemotherapy alone = 5.8 months
- IO + chemotherapy = 8.1 months
1L outcomes in KRAS G12C NSCLC lag behind those with other oncogenic drivers, eg. EGFR and ALK, with available approved targeted therapies.8 Currently available KRAS G12C inhibitors are only approved as single agents for 2L and are limited by challenges with tolerability and durability of response.2,9-11
KRAS G12C Inhibition Downregulates Oncogenesis and Potentially Primes Antitumor Immunity for Favorable Combination with SOC
In preclinical studies, KRAS G12C inhibitors stop oncogenic signaling and reverse some of the immunosuppressive effects in the tumor microenvironment (TME)
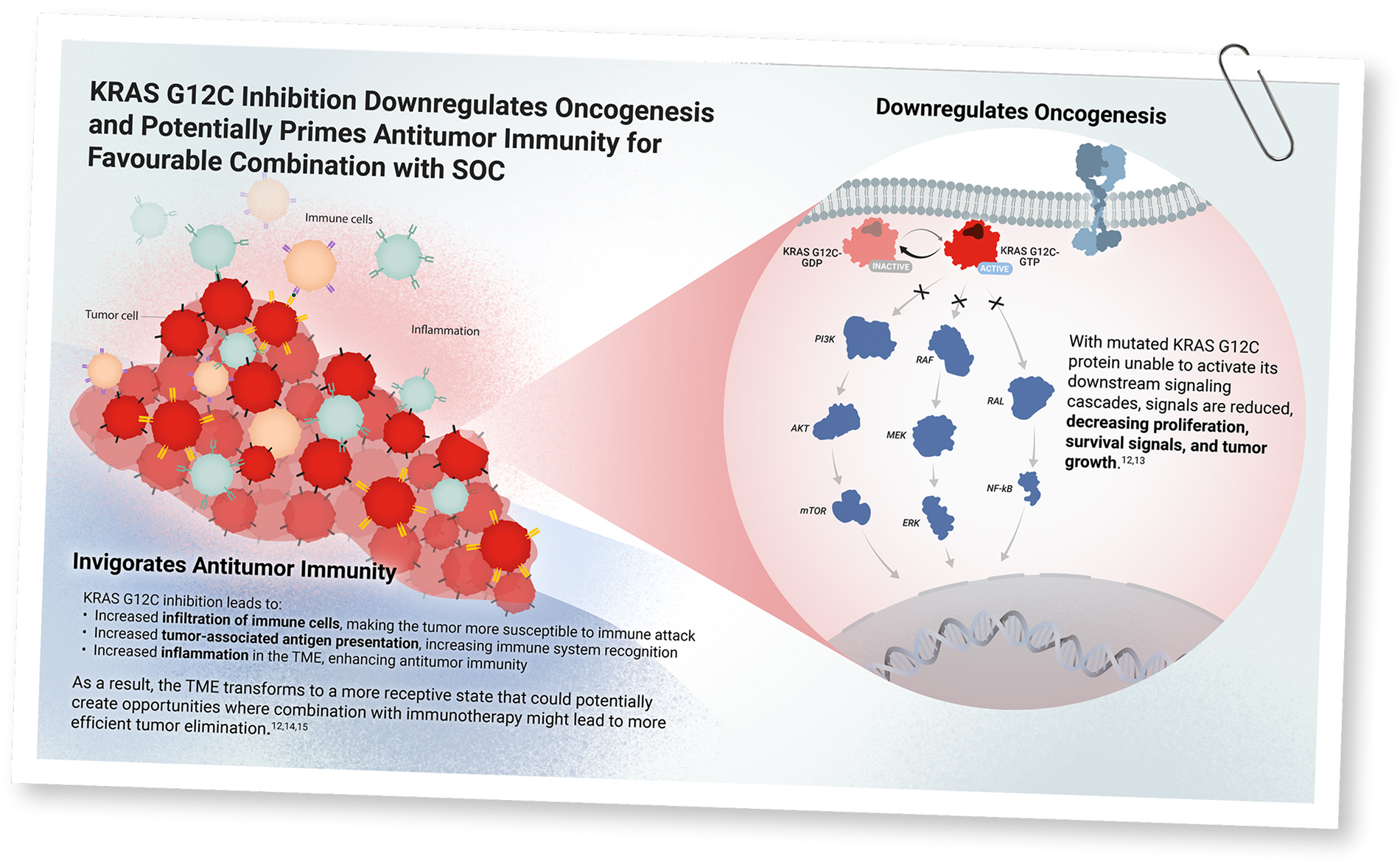
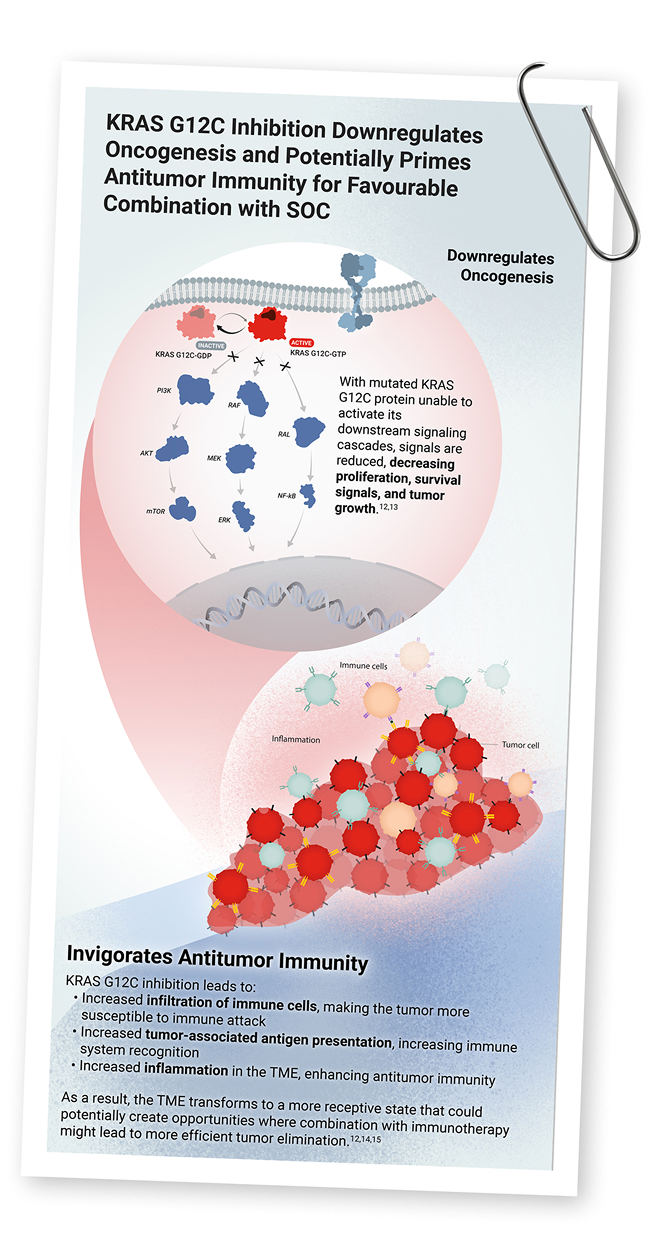
Illustration. Inhibition of KRAS G12C. When KRAS G12C is inhibited it not only reduces downstream signaling pathways, it also reverses the immunosuppressive effects on the tumor microenvironment.
Using KRAS G12C inhibitors may sensitize tumors to respond to IO.15 Meanwhile, chemotherapy rapidly kills dividing cells and reduces tumor burden, limiting the pool of cells that could otherwise develop resistance to KRAS inhibitors.17
Thus, KRAS G12C inhibitors not only directly target the mutated protein, but they may also offer an additive or synergistic immunomodulatory effect with IO, chemotherapy, or chemoimmunotherapy to overcome immune evasion and enhance the ability of the immune system to target and eliminate tumor cells.12,14

A Combination Therapy Approach in 1L Is Emerging

KRAS G12C inhibitors:
- Result in tumor growth inhibition and regression as monotherapy12,13,18,19
- Are synergistic/additive when combined with IO12,14
KRAS G12C inhibitors may demonstrate a manageable safety profile when combined with IO, chemotherapy, or chemoimmunotherapy, with preliminary efficacy data demonstrating benefit metastasis20-24

Phase 3 trials are currently underway to evaluate KRAS G12C inhibitors in combination with IO, chemotherapy, or chemoimmunotherapy. These studies will validate our understanding of integrating KRAS G12C inhibitors with SOC treatments in the 1L setting.25-31
For a patient with KRAS G12C–mutant NSCLC, what does this mean for their care?
KRAS G12C–mutant NSCLC 1L standard of care therapy is typically IO with or without chemotherapy guided by PD-L1 status and other clinical factors such as tumor histology, PD-L1 levels, patient frailty and presence of metastases (eg, brain or liver). While high sensitivity to IO is generally observed, responses may be heterogeneous with rapid disease progression despite treatment. Many patients may not advance to 2L therapy, and current KRAS G12C inhibitors offer modest durability in the 2L+ setting.
Emerging evidence suggests combining KRAS G12C inhibitors with IO, chemotherapy, or chemoimmunotherapy in 1L may enhance immune cell activity and improve treatment responses.
Watch this space for emerging science and updates on KRAS G12C–mutant NSCLC
1L = first line; 2L = second line; ALK = anaplastic lymphoma kinase; CD = cluster of differentiation; EGFR = epidermal growth factor receptor; IO = immunotherapy; KEAP1 = Kelch-like ECH-associated protein 1; KRAS = Kirsten rat sarcoma; MDSC = myeloid-derived suppressor cell; MHC = major histocompatibility complex; NK = natural killer; NRG1 = neuregulin 1; NSCLC = non-small cell lung cancer; OS = overall survival; PD-L1 = programmed death-ligand 1; PFS = progression-free survival; SOC = standard of care; STK11 = serine/threonine kinase 11; TME = tumor microenvironment.
References
- He Q, et al. First-line treatments for KRAS-mutant non-small cell lung cancer: current state and future perspectives. Cancer Biol Ther. 2025;26(1):2441499.
- Cheema PK, et al. Canadian Consensus Recommendations on the Management of KRAS G12C-Mutated NSCLC. Curr Oncol. 2023;30(7):6473-6496.
- Sheffield K, et al. Real-world outcomes with IO and chemo-IO demonstrate unmet need for 1L KRAS G12C-mutant advanced NSCLC in the US. Presented at: IASCL 2025 World Conference on Lung Cancer (WCLC); September 6-9, 2025; Barcelona, Spain. Poster 1615.
- Jaiyesimi IA, et al. Therapy for Stage IV Non-Small Cell Lung Cancer Without Driver Alterations: ASCO Living Guideline, Version 2023.3. J Clin Oncol. 2024;42(11):e23-e43.
- Julian C, et al. Overall survival in patients with advanced non-small cell lung cancer with KRAS G12C mutation with or without STK11 and/or KEAP1 mutations in a real-world setting. BMC Cancer. 2023;23(1):352.
- Wislez M, et al. Real-world effectiveness and tolerability of sotorasib in patients with KRAS G12C-mutated metastatic non-small cell lung cancer: the IFCT-2102 Lung KG12Ci study. Eur J Cancer. 2025;219:115301.
- Esfahanian N, et al. Presentation and outcomes of KRAS G12C mutant non-small cell lung cancer patients with stage IV disease at diagnosis (de novo) versus at recurrence. Cancer Treat Res Commun. 2023:37:100774.
- Lee JK, et al. Comprehensive pan-cancer genomic landscape of KRAS altered cancers and real-world outcomes in solid tumors. NPJ Precis Oncol. 2022;6(1):91.
- Singhal A, et al. Targeting KRAS in cancer. Nat Med. 2024;30(4):969-983.
- Zhang F, et al. Current status of KRAS G12C inhibitors in NSCLC and the potential for combination with anti-PD-(L)1 therapy: a systematic review. Front Immunol. 2025;16:1509173.
- Liu J, et al. The KRAS-G12C inhibitor: activity and resistance. Cancer Gene Ther. 2022;29:875-878.
- Canon J, et al. The clinical KRAS(G12C) inhibitor AMG 510 drives anti-tumour immunity. Nature. 2019;575(7781):217-223.
- Hallin J, et al. The KRASG12C inhibitor MRTX849 provides insight toward therapeutic susceptibility of KRAS-mutant cancers in mouse models and patients. Cancer Discov. 2020;10(1):54-71
- Ni T, et al. Combined inhibition of KRAS G12C and PD-1 boosts the therapeutic efficacy via conditioning of tumor microenvironment in pre-clinical humanized NSCLC mouse models. J Immunother Cancer. 2023;11(Suppl 1):A1-A1731.
- Ghazali N, et al. Immunotherapy in advanced, KRAS G12C-mutant non-small-cell lung cancer: current strategies and future directions. Ther Adv Med Oncol. 2025;17:17588359251323985.
- Huang L, et al. KRAS mutation: from undruggable to druggable in cancer. Signal Transduct Target Ther. 2021;6(1):386.
- Shaverdashvili K, Burns TF. Advances in the treatment of KRASG12C mutant non-small cell lung cancer. Cancer. 2025;131 Suppl 1(Suppl 1):e35783.
- Sabari JK, et al. Activity of adagrasib (MRTX849) in brain metastases: preclinical models and clinical data from patients with KRASG12C-mutant non-small cell lung cancer. Clin Cancer Res. 2022;28(15):3318-3328.
- Brazel D, Nagasaka M. Divarasib in the Evolving Landscape of KRAS G12C Inhibitors for NSCLC. Target Oncol. 2024;19(3):297-301.
- Dragnev KH, et al. Safety and efficacy of olomorasib + immunotherapy in first-line treatment of patients with KRASG12C mutant advanced NSCLC: update from the LOXO-RAS-20001 trial. JCO. 2025;43(suppl).
- Fujiwara Y, et al. Efficacy and safety of olomorasib with pembrolizumab + chemotherapy as first-line treatment in patients with KRAS G12C-mutant advanced NSCLC. JCO. 2024;19(10):S41-S42.
- Sacher AG, et al. MK-1084 for KRAS G12C-mutated (mut) metastatic non–small-cell lung cancer (mNSCLC): results from KANDLELIT-001. J Clin Oncol. 2025;43(Number 16_suppl). ASCO Annual Meeting I abstract 8605.
- Garassino MC, et al. LBA65 KRYSTAL-7: efficacy and safety of adagrasib with pembrolizumab in patients with treatment-naïve, advanced non-small cell lung cancer (NSCLC) harboring a KRASG12C mutation. Ann Oncol. 2023;34:S1309-S1310.
- Negrao MV, et al. Intracranial efficacy of adagrasib in patients from the KRYSTAL-1 trial with KRASG12C-mutated non–small-cell lung cancer who have untreated CNS metastases. J Clin Oncol. 2023;41:4472-4477.
- ClinicalTrials.gov identifier: NCT06793215. Accessed August 28, 2025. https://clinicaltrials.gov/study/NCT06793215?cond=NSCLC
- ClinicalTrials.gov identifier: NCT06345729. Accessed August 28, 2025. https://clinicaltrials.gov/study/NCT06345729?cond=NSCLC
- ClinicalTrials.gov identifier: NCT04613596. Accessed August 28, 2025. https://clinicaltrials.gov/study/NCT04613596?cond=NSCLC
- ClinicalTrials.gov identifier: NCT06119581. Accessed August 28, 2025. https://clinicaltrials.gov/study/NCT06119581?cond=NSCLC
- ClinicalTrials.gov identifier: NCT06875310. Accessed August 28, 2025. https://clinicaltrials.gov/study/NCT06875310?cond=NSCLC
- ClinicalTrials.gov identifier: NCT05920356. Accessed August 28, 2025. https://clinicaltrials.gov/study/NCT05920356?cond=NSCLC
- ClinicalTrials.gov identifier: NCT07190248. Accessed October 6, 2025. https://clinicaltrials.gov/study/NCT07190248?cond=NSCLC
VV-MED-175543
Please rate your satisfaction with the content on the following statements:
Very Dissatisfied
Dissatisfied
Neutral
Satisfied
Very Satisfied