Exposing KRAS G12C: Not Your Usual Suspect in NSCLC
KRAS G12C–Mutant NSCLC Is Unique
KRAS G12C Is a Prevalent Oncogenic Driver Mutation in NSCLC, the Most Common Form of Lung Cancer1,2,4
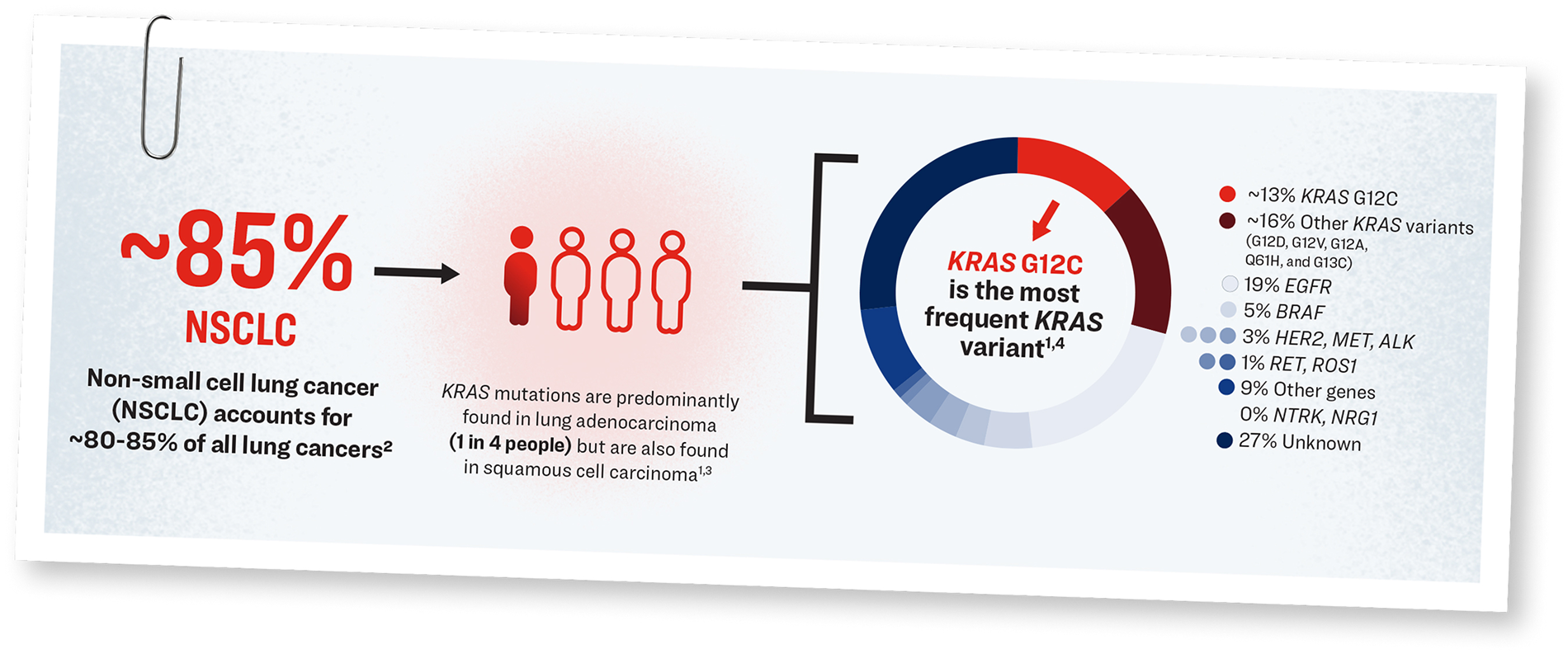
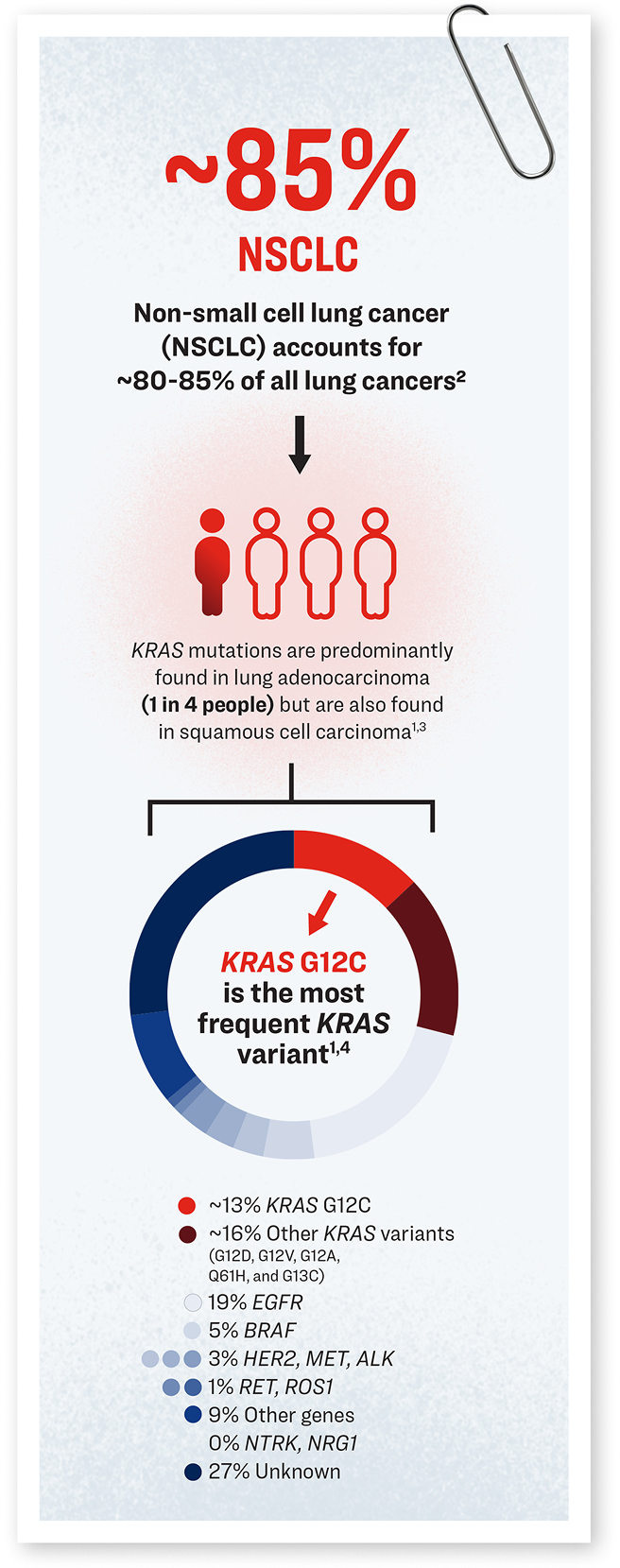
Infographic illustrating the epidemiological landscape of KRAS G12C–mutant NSCLC. NSCLC comprises approximately 85% of all lung cancer diagnoses. Among patients with lung adenocarcinoma—a major NSCLC subtype—approximately 25% harbor KRAS mutations. Within this group, the KRAS G12C variant emerges as the most common mutation.

Patients with KRAS G12C–mutant NSCLC are a heterogenous patient population who typically exhibit a unique profile, with distinct clinical features and tumor characteristics.4,5,7,8,11,14
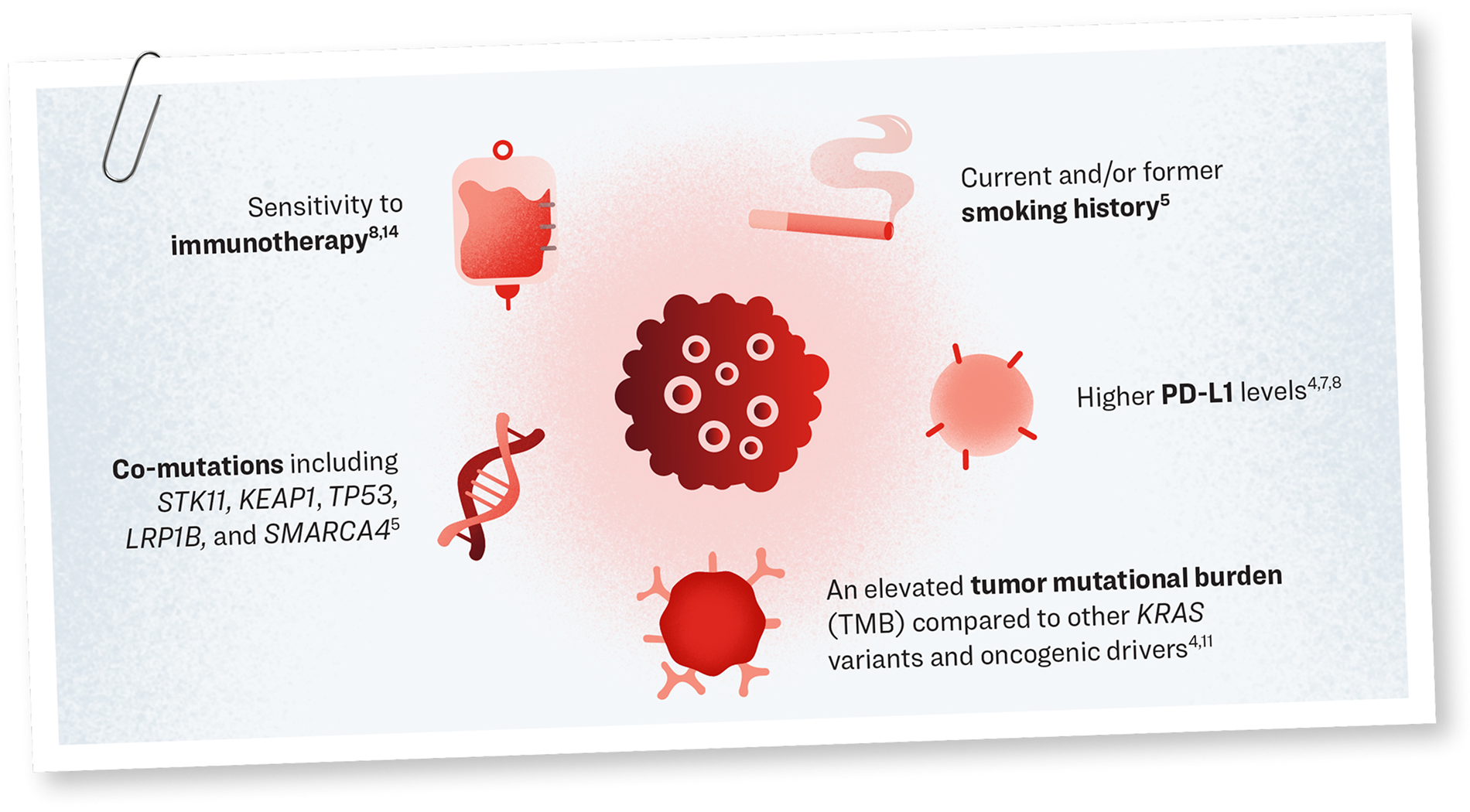
Graphic representation of the unique features that are associated with KRAS G12C tumors, including smoking history, higher PD-L1 levels, an elevated TMB, co-mutations, and sensitivity to immunotherapy.
The KRAS G12C mutation is associated with:
Unlike other oncogenic driver alterations, targeted therapy is not the standard in the first-line (1L) setting:
In KRAS G12C–mutant NSCLC, IO with or without chemotherapy remains the standard of care, with exceptions such as where patients are ineligible for IO/chemotherapy. 1L systemic therapy is often guided by PD-L1 expression.10
KRAS G12C–Mutant NSCLC Is Associated With Poor Prognosis

Poor survival outcomes compared to patients with other oncogenic drivers treated with approved targeted therapies4
Comparable median overall survival (OS) compared to patients with KRAS wild-type tumors when receiving chemotherapy with or without IO with 1L or second-line (2L) treatment17
Most patients had advanced disease at diagnosis
About 25% of patients had documented brain metastasis at the start of 1L treatment
Those treated with 1L chemotherapy + IO treatment had modest median progression-free survival (PFS) of 5 months and OS of 13-16 months
Those with PD-L1 ≥50% treated with 1L IO had a median PFS of 5 months and median OS of 20-22 months
What does having KRAS G12C–mutant NSCLC mean for your patients?
Patients with KRAS G12C–mutant NSCLC are different from patients with NSCLC with other oncogenic drivers.
KRAS G12C mutation is associated with:
- Smoking (current or former)
- Higher PD-L1 levels
- Elevated TMB
- Co-mutations
- General sensitivity to IO
Owing to these unique clinical and tumor characteristics, patients with KRAS G12C–mutant NSCLC may not respond to treatment the same as patients with other oncogenic drivers.
Knowing that patients with KRAS G12C–mutant NSCLC need to be approached differently from your patients with other oncogenic drivers, how might this impact the treatment decisions you make?
Thank you for your participation in this brief knowledge check. It will take less than 3 minutes to complete and is anonymous. Your responses will be aggregated with others and will be non-identifiable.
Explore what underlies the unique characteristics associated with KRAS G12C–mutant NSCLC by continuing to the next section.
This animation visually illustrates the cellular mechanism of disease of KRAS G12C–mutant NSCLC and substantiates the rationale for emerging combination strategies for 1L treatment of KRAS G12C–mutant NSCLC.
00:00 – 00:03
[Background Music]
[Action:] Initial title frame showing corporate logo. Fade in from white. Fade to next frame.
[On screen copy:] Lilly A Medicine Company
00:04 – 00:14
KRAS G12C is a unique oncogenic driver in NSCLC and is associated with poor prognosis.1-5
[Action:] Main title frame showing the animation title fades in, with the text appearing after the overlay.
[On screen copy:] KRAS G12C: a Unique Oncogenic Driver in NSCLC
00:15 – 00:18
[Action:] The overlay scales down, and the chapter title appears. It then fades away as the camera rack focuses on the scene behind.
[On screen copy:] Introduction to KRAS in NSCLC
00:19 – 00:27
Many patients with lung adenocarcinoma have KRAS mutations, with the KRAS G12C variant being the most common.6-7
[Action:] Camera zooms in slowly as model turns clockwise and the copy appears.
[On screen copy:] In patients diagnosed with NSCLC, ~30% have KRAS mutations7,*
*Depending on geography for overall patient population, regardless of gender.6
00:28 – 00:32
Tumors with KRAS G12C mutations are different than tumors with...3-5
[Action:] Text fades in from right. Thorax goes semitransparent, revealing lungs with NSCLC. Text fades out.
[On screen copy:] Tumors with KRAS G12C mutations are different3-5
00:33 – 00:41
...other oncogenic drivers and have unique clinicopathological characteristics and biological heterogeneity that can lead to varied response to therapy.1, 3-5, 8
[Action:] Icons fade in from the right in the order of top to bottom. After narration finishes, icons disappear, leaving the model with visible lungs on screen. Frame fades to next frame.
[On screen copy:] Unique Features of KRAS G12C–Mutant NSCLC
[On screen label:]
- Smoking: current or previous1,8
- PD-L1: higher levels2, 3, 5, *
- Tumor Mutation Burden: higher2, 4, *
- Co-mutations: common1, 8
- Immunotherapy: higher sensitivity5, 9, *
*Compared to NSCLC tumors with other oncogenic driver alterations.3-5
00:42 – 00:49
KRAS normally acts as an intracellular molecular switch, regulating downstream signaling pathways...10
[Action:] Camera is focused on the rightmost KRAS. The left KRAS is glowing but out of focus. GTP binds to KRAS while GDP unbinds.
[On screen label:] KRAS
00:50 – 00:53
...by cycling between an active GTP-bound state...10
[On screen label:] Active KRAS, GTP
00:54 – 00:56
...and an inactive GDP-bound state.10
[Action:] Camera shifts focus to the KRAS on the left (foreground). It deactivates.
[On screen label:] Inactive KRAS, GDP
00:57 – 01:05
Activation of KRAS occurs by the binding of signal ligands to different receptor tyrosine kinases at the cell membrane.7, 11
[Action:] Camera trucks to the left to show more membrane. RTKs move in from off screen during camera movement.
[On screen label:] Ligand, RTK (eg, EGFR, ALK, ROS1)
01:06 – 01:08
Ligand binding triggers GDP release,...11
[Action:] RTK complex is “energized” and then influences KRAS.
[On screen label:] Inactive KRAS, GDP, GTP
01:09 – 01:17
...enabling GTP to bind, driving a conformational change, which activates the protein.11
[Action:] GTP binds, leading to a conformational change. KRAS is “energized.”
[On screen label:] Active KRAS
01:18 – 01:24
GTP-bound KRAS transmits signals that recruit and activate downstream signaling pathways,...10-12
[Action:] Camera zooms out and jibs down to reveal more intracellular space and a part of the nucleus. Glow effect propagates down pathways.
[On screen label:] Active KRAS, PI3K, AKT, mTOR, RAF, MEK, ERK, RAL, NF-kB, Nucleus
01:25 – 01:29
...regulating proliferation, apoptosis, differentiation, and cell survival.7, 11
[Action:] Scene becomes blurry, overlay icons appear.
[On screen label:] Proliferation, Apoptosis, Differentiation, Cell Survival
01:30 – 01:34
[Action:] Overlay appears with text, then fades away, revealing and focusing on the scene behind.
[On screen copy:] KRAS G12C Mutation as a Driver and Evader
01:35 – 01:48
A single point missense mutation in KRAS codon 12 leads to the substitution of glycine with cysteine, resulting in KRAS G12C protein, which is a variant of KRAS protein.7, 11, 13
[Action:] Camera focuses on the rightmost new KRAS G12C. When mutation is mentioned, the Cys12 glowing area pulses.
[On screen label:] KRAS G12C, GTP, Cys12 mutation
01:49
[Action:] Show conformational change, with pocket forming (light green dotted area).
01:50 – 02:05
The substituted cysteine impairs GTP hydrolysis, causing KRAS G12C to be predominantly in the GTP-bound active state.10, 11, 13
[Action:] Other KRAS molecules highlight Cys12 region, turn green, cycle ON/OFF. Rapid cycling shows impaired hydrolysis.
02:06 – 02:17
Constitutively activated KRAS G12C exerts two key effects. The first is a loss of regulation of downstream pathways,...10, 11, 13
[Action:] Zoom out, truck right to show pathway again. Signaling pulses rapidly.
[On screen copy:] Deregulation of downstream pathways
[On screen label:] Active KRAS G12C, PI3K, AKT, mTOR, RAF, MEK, ERK, RAL, NF-kB, Nucleus
02:18 – 02:23
...resulting in uncontrolled cell proliferation and increased cell survival, leading to tumor formation.10, 11, 13
[Action:] Show tumor forming on lung tissue.
[On screen label:] Tumor formation
02:24 – 02:28
Second, it affects the tumor microenvironment by recruiting suppressive immune cells,...3, 14
[Action:] Immune cells move onto tumor surface.
[On screen title:] KRAS G12C-Mutant NSCLC Tumor Microenvironment
[On screen label:] Recruit suppressive immune cells, Regulatory T cells, Myeloid-derived suppressor cells
02:29 – 02:32
...upregulating PD-L1,...3,14
[Action:] Proteins appear on tumor surface, strengthening force field.
[On screen label:] PD-L1 upregulation, PD-L1
02:33 – 02:39
...and excluding antitumor immune cells, enabling immune evasion and enhanced tumor survival.3, 14
[Action:] Antitumor immune cells expelled by force field.
[On screen label:] Exclude antitumor immune cells, Antitumor immune cells, PD-L1
02:40 – 02:46
[Action:] Overlay appears with text, then fades away.
[On screen copy:] Inhibition of KRAS G12C to Promote Antitumor Response
02:47 – 02:56
KRAS G12C was once thought to be undruggable due to structural and functional complexities that prevented binding of pharmacological molecules.10, 13
[Action:] KRAS G12C cycles slowly, inhibitors bounce away.
[On screen label:] KRAS G12C, Cys12 mutation, GTP, GDP, KRAS G12C inhibitor
02:57 – 03:10
Thanks to scientific advances, KRAS G12C is now druggable, and the binding of inhibitors traps the mutated protein in the inactive GDP-bound state.10, 15
[Action:] Cycling stops, KRAS G12C trapped inactive.
[On screen copy (footnote):] Multiple mechanisms of KRAS G12C inhibition are under investigation.10
03:11 – 03:19
This reduces the effects of KRAS G12C on downstream signaling pathways, decreasing proliferation and increasing cell apoptosis.16-20
[Action:] Signals fade almost completely.
[On screen label:] Inactive KRAS G12C, PI3K, AKT, mTOR, RAF, MEK, ERK, RAL, NF-kB, Nucleus
03:20 – 03:30
Additionally, KRAS G12C inhibition reshapes the tumor microenvironment, increasing immune cell infiltration, tumor-associated antigen presentation,...9, 14, 16
[Action:] Force field destroyed, immune cells aggregate, tumor shrinks.
[On screen title:] KRAS G12C Inhibition Reshapes the Tumor Microenvironment
[On screen label:] Immune cell infiltration, Antigen presentation, PD-L1
03:31 – 03:35
...and inflammation, thereby enhancing immunogenicity and antitumor response.9, 14, 16
[Action:] Heat distortion, tumor shrinking.
[On screen label:] Inflammation
03:36 – 03:56
Preclinical data suggest that KRAS G12C inhibitors directly target the mutated protein and may offer an additive or synergistic effect with immunotherapy or chemotherapy to overcome immune evasion and enhance the ability of the immune system to target and eliminate tumor cells.16-20
[Action:] Tumor shrinks rapidly but not fully disappears.
[On screen copy:] KRAS G12C inhibitors may offer an additive or synergistic effect with immunotherapy or chemotherapy.16-20
03:57 – 04:12
Ongoing Phase 3 trials are combining KRAS G12C inhibitors with immunotherapy, chemotherapy, or chemoimmunotherapy as a new strategy for first-line treatment of advanced KRAS G12C–mutant NSCLC.21-26
[Action:] KRAS hero molecule spotlighted.
[On screen copy:] Ongoing Phase 3 trials are evaluating KRAS G12C inhibitors in combination with immunotherapy, chemotherapy, or chemoimmunotherapy for first-line treatment of KRAS G12C–mutant NSCLC.21-26
04:13 – 04:32
[On screen copy:]
Abbreviations:
AKT = protein kinase B; ALK = anaplastic lymphoma kinase; Cys12 = cysteine 12; EGFR = epidermal growth factor receptor; ERK = extracellular signal-regulated kinase; GDP = guanosine diphosphate; GTP = guanosine triphosphate; KRAS = Kirsten rat sarcoma; MEK = mitogen-activated protein kinase; mTOR = mammalian target of rapamycin; NF-kB = nuclear factor-kB; NSCLC = non-small cell lung cancer; PD-L1 = programmed death-ligand 1; PI3K = phosphatidylinositol 3-kinase; RAF = rapidly accelerated fibrosarcoma; RAL = Ras-like protein; ROS1 = ROS Proto-Oncogene 1.
References:
- Sheffield K, et al. Real-world outcomes with IO and chemo-IO demonstrate unmet need for 1L KRAS G12C-mutant advanced NSCLC in the US. IASCL 2025 World Conference on Lung Cancer (WCLC); September 6-9, 2025; Barcelona, Spain. Poster 1615.
- Lee JK, et al. Comprehensive pan-cancer genomic landscape of KRAS altered cancers and real-world outcomes in solid tumors. NPJ Precis Oncol. 2022;6(1):91.
- Xu M, et al. Unveiling the role of KRAS in tumor immune microenvironment. Biomed & Pharmacother. 2024;171:116058.
- Negrao MV, et al. Oncogene-specific differences in tumor mutational burden, PD-L1 expression, and outcomes from immunotherapy in non-small cell lung cancer. J Immunother Cancer. 2021;9(8):e002891.
- Alsaed B, et al. Shaping the battlefield: EGFR and KRAS tumor mutations' role on the immune microenvironment and immunotherapy responses in lung cancer. Cancer Metastasis Rev. 2025;44(3):56.
- Acker F, et al. KRAS mutations in squamous cell carcinomas of the lung. Front Oncol. 2021;11:788084.
- Chevallier M, et al. Oncogenic driver mutations in non-small cell lung cancer: past, present and future. World J Clin Oncol. 2021;12(4):217-237.
- Salem ME, et al. Landscape of KRAS G12C, associated genomic alterations, and interrelation with immuno-oncology biomarkers in KRAS-mutated cancers. JCO Precis Oncol. 2022;6:e2100245.
- Ghazali N, et al. Immunotherapy in advanced, KRAS G12C-mutant non-small-cell lung cancer: current strategies and future directions. Ther Adv Med Oncol. 2025;17:17588359251323985.
- Singhal A, et al. Targeting KRAS in cancer. Nat Med. 2024;30(4):969-983.
- Ferreira A, et al. Crucial role of oncogenic KRAS mutations in apoptosis and autophagy regulation: therapeutic implications. Cells. 2022;11(14):2183.
- Fu S, et al. Precision immune regulation in KRAS-mutated cancers: the final piece of the puzzle? J Exp Clin Cancer Res. 2025;44(1):189.
- Lim TKH, et al. KRAS G12C in advanced NSCLC: prevalence, co-mutations, and testing. Lung Cancer. 2023;184:107293.
- Huang L, et al. KRAS mutation: from undruggable to druggable in cancer. Signal Transduct Target Ther. 2021;6(1):386.
- Ostrem, JM, et al. K-Ras(G12C) inhibitors allosterically control GTP affinity and effector interactions. Nature. 2013;503:548-551.
- Canon J, et al. The clinical KRAS(G12C) inhibitor AMG 510 drives anti-tumour immunity. Nature. 2019;575(7781):217-223.
- Hallin J, et al. The KRASG12C inhibitor MRTX849 provides insight toward therapeutic susceptibility of KRAS-mutant cancers in mouse models and patients. Cancer Discov. 2020;10(1):54-71.
- Ni T, et al. Combined inhibition of KRAS G12C and PD-1 boosts the therapeutic efficacy via conditioning of tumor microenvironment in pre-clinical humanized NSCLC mouse models. J Immunother Cancer. 2023;11(Suppl 1):A1-A1731.
- Sabari JK, et al. Activity of adagrasib (MRTX849) in brain metastases: preclinical models and clinical data from patients with KRASG12C-mutant non-small cell lung cancer. Clin Cancer Res. 2022;28(15):3318-3328.
- Brazel D, Nagasaka M. Divarasib in the Evolving Landscape of KRAS G12C Inhibitors for NSCLC. Target Oncol. 2024;19(3):297-301.
- ClinicalTrials.gov identifier: NCT06793215. Accessed August 28, 2025. https://clinicaltrials.gov/study/NCT06793215?cond=NSCLC
- ClinicalTrials.gov identifier: NCT06345729. Accessed August 28, 2025. https://clinicaltrials.gov/study/NCT06345729?cond=NSCLC
- ClinicalTrials.gov identifier: NCT04613596. Accessed August 28, 2025. https://clinicaltrials.gov/study/NCT04613596?cond=NSCLC
- ClinicalTrials.gov identifier: NCT06119581. Accessed August 28, 2025. https://clinicaltrials.gov/study/NCT06119581?cond=NSCLC
- ClinicalTrials.gov identifier: NCT06875310. Accessed August 28, 2025. https://clinicaltrials.gov/study/NCT06875310?cond=NSCLC
- ClinicalTrials.gov identifier: NCT05920356. Accessed August 28, 2025. https://clinicaltrials.gov/study/NCT05920356?cond=NSCLC
04:33 – 04:42
[Action:] End slate, Lilly corporate title/logo
[On screen copy:] VV-MED-175771 ©2025 Eli Lilly and Company. All rights reserved.
Hear from Dr. Martin F. Dietrich and Dr. Bruna Pellini about why patients with KRAS G12C–mutant NSCLC need to be approached differently and how combination strategies are emerging in 1L for these patients.
00:00 – 00:06
Audio: [Background music]
[Actions]: Initial title frame fades in.
[On-screen text]: Clinical Perspectives: Tailored Treatment Approaches for KRAS G12C–Mutant NSCLC; Presented by Martin F. Dietrich, MD, PhD (US Oncology Network and the University of Central Florida) and Bruna Pellini, MD (Chief of Thoracic Oncology, Miami Cancer Institute – Baptist Health South Florida); Lilly logo.
00:07 – 00:26
Dr. Dietrich: Today, we will explore what makes KRAS G12C a unique oncogenic driver in non-small cell lung cancer and what implications this has on treatment outcomes.
Dr. Pellini: We will also delve deeper into understanding emerging approaches for first-line treatment of KRAS G12C–mutant metastatic non-small cell lung cancer.
[Actions]: Medium close-up of both speakers; chapter headings animate as each speaks.
[On-screen text]: Chapter 1: Patients With KRAS G12C–Mutant NSCLC Have a Unique Profile; Chapter 2: Patients With KRAS G12C–Mutant NSCLC Have Poor Survival Outcomes; Chapter 3: Emerging Combinations for 1L Treatment of KRAS G12C–Mutant NSCLC.
00:26 – 00:38
Audio: —
[Actions]: Disclaimer scene begins.
[On-screen text]: Disclaimer:
Dr. Martin F. Dietrich is a clinical researcher and community oncologist. He provides consulting, speaking, and other professional services for Lilly.
Dr. Bruna Pellini is a thoracic medical oncologist. She receives speaker honoraria and serves on advisory boards and scientific steering committees for Lilly.
They both have been compensated by Lilly to speak on clinical perspectives in KRAS G12C–mutant non-small cell lung cancer.
This presentation was created by Lilly Medical and is intended to be used by HCPs for medical, scientific, and educational purposes.
00:39 – 00:45
Audio: —
[Actions]: Title frame reappears.
[On-screen text]: Clinical Perspectives: Tailored Treatment Approaches for KRAS G12C–Mutant NSCLC.
00:46 – 01:13
Audio: Dr. Dietrich:Hello! I’m Dr. Dietrich and I maintain an active clinical research practice in a community setting. In my practice, I focus on patients with advanced non-small cell lung cancer. I see about 15 patients with KRAS G12C–mutant non-small cell lung cancer in a year.
Dr. Pellini:Hello, I’m Dr. Pellini and I’m deeply involved in translational research. In my clinic, I see about 100 patients with advanced non-small cell lung cancer every month and about 30 new patients with KRAS G12C–mutant non-small cell lung cancer every year.
[Actions]: Medium shot → name cards animate → close-ups for each speaker.
[On-screen text]: Martin F. Dietrich, MD, PhD
US Oncology Network and the University of Central Florida Bruna Pellini, MD Chief of Thoracic Oncology Miami Cancer Institute – Baptist Health South Florida
01:14 – 01:19
[Actions]: Chapter 1 title screen.
[On-screen text]: Chapter 1: Patients With KRAS G12C–Mutant NSCLC Have a Unique Profile.
01:20 – 01:38
Audio: Dr. Pellini:
The literature shows that patients with KRAS G12C–mutant NSCLC are different from patients with other oncogenic drivers.
Dr. Dietrich, what are the distinct clinical features and tumor characteristics that make patients with NSCLC with a KRAS G12C mutation unique?
[Actions]: Medium shot → close-up of Pellini.
01:39 – 01:56
Audio: Dr. Dietrich explains smoking history, PD-L1 levels, tumor mutational burden, and co-mutations.
[Actions]: Full-screen icon animation.
[On-screen text]: Key characteristics including smoking history, higher PD-L1, elevated TMB, and co-mutations (STK11, KEAP1, TP53, LRP1B, SMARCA4).
01:57 – 02:19
Audio: Dr. Dietrich explains how PD-L1 and TMB influence immunogenicity and sensitivity to immunotherapy.
[Actions]: Medium shot → close-up with icon/text animation.
[On-screen text]: Sensitivity to immunotherapy.
02:20 – 02:22
[On-screen text]:
References
- Salem ME, et al. Landscape of KRAS G12C, associated genomic alterations, and interrelation with immuno-oncology biomarkers in KRAS-mutated cancers. JCO Precis Oncol. 2022;6:e2100245.
- Xu M, et al. Unveiling the role of KRAS in tumor immune microenvironment. Biomed & Pharmacother. 2024;171:116058.
- Alsaed B, et al. Shaping the battlefield: EGFR and KRAS tumor mutations' role on the immune microenvironment and immunotherapy responses in lung cancer. Cancer Metastasis Rev. 2025;44(3):56.
- Lee JK, et al. Comprehensive pan-cancer genomic landscape of KRAS altered cancers and real-world outcomes in solid tumors. NPJ Precis Oncol. 2022;6(1):91.
- Negrao MV, et al. Oncogene-specific differences in tumor mutational burden, PD-L1 expression, and outcomes from immunotherapy in non-small cell lung cancer. J Immunother Cancer. 2021;9(8):e002891.
- Ghazali N, et al. Immunotherapy in advanced, KRAS G12C-mutant non-small-cell lung cancer: current strategies and future directions. Ther Adv Med Oncol. 2025;17:17588359251323985.
- Borg M, et al. Four decades of lung cancer: trends in comorbidities and causes of death in a nationwide Danish cohort. Eur J Cancer. 2025.218:115303.
- Wu L, et al. Pan-cancer analysis to character the clinicopathological and genomic features of KRAS-mutated patients in China. J Cancer Res Clin Oncol. 2025;151(2):94
02:23 – 02:26
[Actions]: Chapter 2 title screen.
[On-screen text]: Chapter 2: Patients With KRAS G12C–Mutant NSCLC Have Poor Survival Outcomes.
02:27 – 02:47
Audio: Dr. Dietrich: Unlike most other driver alterations, KRAS G12C mutations are more responsive to immunotherapy, and, in fact, it is currently the first-line standard of care either by itself or in combination with chemotherapy, depending on PD-L1 expression and other patient and tumor characteristics.1-3
Doctor Pellini, I’m curious what real-world outcomes do you see in these patients?
[Actions]: Open on medium shot of the TLs facing each other. Cut to closeup of Dietrich with icon and text animation. When Dietrich questions Pellini, the camera cuts back to the medium shot of the TLs facing each other.
[On-screen text]: SOC Immunotherapy with or without chemotherapy.
02:48 – 03:02
Audio: Dr. Pellini: I would say, generally, these patients have poor outcomes. Their overall survival is shorter than that of patients with other targetable driver alterations with available targeted therapies in the first-line setting.4 And most patients have advanced disease at diagnosis.
[Actions]: Cut to medium closeup of Pellini. Text and icon animate on screen.
[On-screen text]: Treatment with 1L chemo + IO:
- mPFS = 5 months
- OS = 13-16 months
03:03 – 03:12
Audio: Dr. Pellini: Unfortunately, about a quarter of patients have brain metastasis at the start of first-line treatment, and about 40% may develop them over their lifetime.4,5
[Actions]: Stay on medium closeup of Pellini with text and icon animation.
[On-screen text]:
- 25% at start of 1L;
- 40% during lifetime.
03:13 – 03:19
Audio: Dr. Dietrich: We do, though, have targeted therapies approved for use after first-line treatment of immunotherapy, with or without chemotherapy.2,6
[Actions]: Cut to medium shot of TLs facing each other.
[On-screen text]: —
03:20 – 03:45
Audio: Dr. Pellini
Yes. However, less than 40% of our patients continue on to receive second-line therapy for a variety of reasons including performance status and frailty.4,7
Overall, patient outcomes following first-line therapy in KRAS G12C–mutant NSCLC lag behind those we see with other oncogenic drivers with available approved targeted therapies, such as EGFR and ALK.8
[Actions]: Cut to medium closeup of Pellini with text and icon animation.
[On-screen text]: Only 38% of patients receive 2L
Effective and well-tolerated treatment remains an unmet need in the 1L setting for
KRAS G12C–mutant NSCLC
03:46 – 03:46
[On-screen text]:
References
- He Q, et al. First-line treatments for KRAS-mutant non-small cell lung cancer: current state and future perspectives. Cancer Biol Ther. 2025;26(1):2441499.
- Cheema PK, et al. Canadian consensus recommendations on the management of KRAS G12C-mutated NSCLC. Curr Oncol. 2023;30(7):6473-6496.
- Mazieres J, et al. Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: results from the IMMUNOTARGET registry. Ann Oncol. 2019;30(8):1321-1328.
- Sheffield K, et al. Real-world outcomes with IO and chemo-IO demonstrate unmet need for 1L KRAS G12C-mutant advanced NSCLC in the US. Presented at: IASCL 2025 World Conference on Lung Cancer (WCLC); September 6-9, 2025; Barcelona, Spain. Poster 1615.
- Sabari JK, et al. Activity of adagrasib (MRTX849) in brain metastases: preclinical models and clinical data from patients with KRASG12C-mutant non-small cell lung cancer. Clin Cancer Res. 2022;28(15):3318-3328.
- Singhal A, et al. Targeting KRAS in cancer. Nat Med. 2024;30(4):969-983.
- Esfahanian N, et al. Presentation and outcomes of KRASG12C mutant non-small cell lung cancer patients with stage IV disease at diagnosis (de novo) versus at recurrence. Cancer Treat Res Commun. 2023:37:100774.
- Lee JK, et al. Comprehensive pan-cancer genomic landscape of KRAS altered cancers and real-world outcomes in solid tumors. NPJ Precis Oncol. 2022;6(1):91.
03:47 – 03:53
[Actions]: Chapter 3 title screen.
[On-screen text]: Chapter 3: Emerging Combinations for 1L Treatment of KRAS G12C–Mutant NSCLC.
03:54 – 04:12
Audio: Dr. Dietrich: To understand the challenges with using first-line immunotherapy with or without chemotherapy in advanced NSCLC and the possibilities with emerging treatment strategies we should look at the KRAS G12C mutation more closely
Dr. Pellini, can you share what happens at the cellular level in a KRAS G12C–mutant tumor?
[Actions]: Open on medium shot of TLs facing each other.
04:13 – 04:18
Audio: Dr. Pellini: Well, KRAS is an intracellular protein that regulates normal cellular processes.1
[Actions]: Cut to closeup of Pellini. Soon after she begins speaking, the screen changes to 3D animation clips of the intracellular processes.
[On-screen text]: Active KRAS
AKT
ERK
MEK
mTOR
NF-κB
Nucleus
PI3K
RAF
RAL
04:19 – 04:31
Audio: Dr. Pellini: When mutated, KRAS G12C becomes constitutively active, driving oncogenesis. This mutated protein also supports immune evasion by tumor cells, creating a favorable environment for tumor survival.1-6
[Actions]: The screen shows 3D animation clips of the intracellular processes. Cut to closeup of Pellini. Soon after she begins speaking, the screen changes to a 3D visualization of GTP-bound KRAS.
[On-screen text]: Active KRAS G12C
AKT
ERK
MEK
mTOR
NF-κB
Nucleus
PI3K
RAF
RAL
Deregulation of downstream pathways
GTP-bound KRAS
- Tumor formation
- Recruit suppressive immune cells
- PD-L1 upregulation
- Exclude antitumor immune cells
04:32 – 04:44
Audio: Dr. Pellini: In fact, preclinical studies are showing that inhibiting KRAS G12C stops oncogenic signaling and appears to reverse some of the immunosuppressive effects in the tumor microenvironment.7-10
[Actions]: The screen Dietrich and Pellini speaking. Cut to 3D animation clips of the intracellular processes. Soon after, the screen changes to a 3D visualization of KRAS G12C interacting with the environment.
[On-screen text]: AKT
ERK
Inactive KRAS
G12C
MEK
mTOR
NF-κB
Nucleus
PI3K
RAF
RAL
Multiple mechanisms of inhibition of KRAS G12C are under investigation.
KRAS G12C reshapes tumor microenvironment
- Immune cell infiltration
- Antigen presentation
- Inflammation
04:45 – 04:59
Audio: Dr. Pellini: As a result, the tumor microenvironment transforms to a more receptive state. It could potentially create opportunities where combining a KRAS G12C inhibitor with immunotherapy and/or chemotherapy might lead to improved outcomes.7,11
[Actions]: Cut back to the medium closeup shot of Pellini.
05:00 – 05:16
Audio: Dr. Pellini: More importantly, Phase 1 and 2 data with certain KRAS G12C inhibitors have shown that they can be combined with immunotherapy and/or chemotherapy, with a manageable safety profile in patients with metastatic NSCLC.12-16
[Actions]: Cut to medium closeup of Pellini with text and icon animation.
[On-screen text]: Preliminary efficacy data demonstrate an impact that includes brain metastasis.
05:17 – 05:30
Audio: Dr. Dietrich: That is very interesting, and I understand we now have Phase 3 trials underway that will further advance our understanding of integrating KRAS G12C inhibitors with immunotherapy and/or chemotherapy in the first-line setting in metastatic NSCLC.17-23
[Actions]: Cut to medium closeup of Dietrich with text and icon animation.
[On-screen text]: Ongoing Phase 3 trials.
05:31 – 05:59
Audio: Dr. Pellini: Today we saw that beyond its unique biology, KRAS G12C impacts outcomes because it modulates the tumor microenvironment.
Its inhibition is now being evaluated in combination with immunotherapy and/or chemotherapy for greater benefit.
Dr. Dietrich: It’s been a pleasure sharing our perspectives on KRAS G12C–mutant non-small cell lung cancer, and we look forward to continuing this important conversation as more data emerge. Thanks for watching.
[Actions]: Cut to a medium shot of both TLs together.
06:00 – 06:05
[Actions]: Reference screen.
[On-screen text]:
References
- Singhal A, et al. Targeting KRAS in cancer. Nat Med. 2024;30(4):969-983.
- Ferreira A, et al. Crucial role of oncogenic KRAS mutations in apoptosis and autophagy regulation: therapeutic implications. Cells. 2022;11(14):2183.
- Huang L, et al. KRAS mutation: from undruggable to druggable in cancer. Signal Transduct Target Ther. 2021;6(1):386.
- Lim TKH, et al. KRAS G12C in advanced NSCLC: prevalence, co-mutations, and testing. Lung Cancer. 2023;184:107293.
- Xu M, et al. Unveiling the role of KRAS in tumor immune microenvironment. Biomed & Pharmacother. 2024;171:116058.
- Karimi N, Moghaddam SJ. KRAS-mutant lung cancer: Targeting molecular and immunologic pathways, therapeutic advantages and restrictions. Cells. 2023;12(5):749.
- Canon J, et al. The clinical KRAS(G12C) inhibitor AMG 510 drives anti-tumour immunity. Nature. 2019;575(7781):217-223.
- Sabari JK, et al. Activity of adagrasib (MRTX849) in brain metastases: preclinical models and clinical data from patients with KRASG12C-mutant non-small cell lung cancer. Clin Cancer Res. 2022;28(15):3318-3328.
- Brazel D, Nagasaka M. Divarasib in the evolving landscape of KRAS G12C inhibitors for NSCLC. Target Oncol. 2024;19(3):297-301.
- Hallin J, et al. The KRASG12C inhibitor MRTX849 provides insight toward therapeutic susceptibility of KRAS-mutant cancers in mouse models and patients. Cancer Discov. 2020;10(1):54-71.
- Ni T, et al. Combined inhibition of KRAS G12C and PD-1 boosts the therapeutic efficacy via conditioning of tumor microenvironment in pre-clinical humanized NSCLC mouse models. J Immunother Cancer. 2023;11(Suppl 1):A1-A1731.
- Dragnev KH, et al. Safety and efficacy of olomorasib + immunotherapy in first-line treatment of patients with KRASG12C mutant advanced NSCLC: update from the LOXO-RAS-20001 trial. JCO. 2025;43(suppl).
- Fujiwara Y, et al. Efficacy and safety of olomorasib with pembrolizumab + chemotherapy as first-line treatment in patients with KRAS G12C-mutant advanced NSCLC. JCO. 2024;19(10):S41-S42.
- Sacher AG, et al. MK-1084 for KRAS G12C-mutated (mut) metastatic non–small-cell lung cancer (mNSCLC): results from KANDLELIT-001. J Clin Oncol. 2025;43(Number 16_suppl). ASCO Annual Meeting I abstract 8605.
- Garassino MC, et al. LBA65 KRYSTAL-7: efficacy and safety of adagrasib with pembrolizumab in patients with treatment-naïve, advanced non-small cell lung cancer (NSCLC) harboring a KRASG12C mutation. Ann Oncol. 2023;34:S1309-S1310.
- Li BT, et al. Sotorasib plus carboplatin and pemetrexed in KRAS G12C advanced NSCLC: updated analysis from the international CodeBreaK 101 trial. J Clin Oncol. 2024;42(16_suppl):8512.
- ClinicalTrials.gov identifier: NCT06793215. Accessed September 11, 2025. https://clinicaltrials.gov/study/NCT06793215?cond=NSCLC
- ClinicalTrials.gov identifier: NCT06345729. Accessed September 11, 2025. https://clinicaltrials.gov/study/NCT06345729?cond=NSCLC
- ClinicalTrials.gov identifier: NCT04613596. Accessed September 11, 2025. https://clinicaltrials.gov/study/NCT04613596?cond=NSCLC
- ClinicalTrials.gov identifier: NCT06119581. Accessed September 11, 2025. https://clinicaltrials.gov/study/NCT06119581?cond=NSCLC
- ClinicalTrials.gov identifier: NCT06875310. Accessed September 11, 2025. https://clinicaltrials.gov/study/NCT06875310?cond=NSCLC
- ClinicalTrials.gov identifier: NCT05920356. Accessed September 11, 2025. https://clinicaltrials.gov/study/NCT05920356?cond=NSCLC
- ClinicalTrials.gov identifier: NCT07190248. Accessed October 6, 2025. https://clinicaltrials.gov/study/NCT07190248?cond=NSCLC
06:06 – 06:15
Audio: —
[Actions]: Static screen.
[On-screen text]: ON-SCREEN TEXT:
Conflicts of interest
Martin F. Dietrich, MD, PhD
Consulting:
Amgen
AstraZenecaBayer
BeOne Oncology
Boehringer Ingelheim
Blueprint Medicines
Bristol Myers Squibb
Caris Life Sciences
Daiichi Sankyo
Eli Lilly
EMD Serono
Epizyme
Foundation Medicine
G1 Therapeutics
Genentech
Gilead Pharmaceuticals
Janssen Pharmaceuticals
Mirati Therapeutics
Myriad
Novartis
Nuvalent
Nuvation Bio
Pfizer
Puma
Regeneron
Sanofi Genzyme
Stemline Oncology
Takeda
Speaking/Services other than consulting:
Amgen
AstraZeneca
Bayer
BeOne Oncology
Boehringer Ingelheim
Blueprint Medicines
Bristol Myers Squibb
Caris Life Sciences
Daiichi Sankyo
Eli Lilly
EMD Serono
Epizyme
Foundation Medicine
G1 Therapeutics
Genentech
Gilead Pharmaceuticals
Janssen Pharmaceuticals
Mirati Therapeutics
Myriad
Novartis
Nuvalent
Pfizer
Pharmacosmos
Puma
Regeneron
Sanofi Genzyme
Stemline Oncology
Takeda
Ownership:
CrossBridge Therapeutics, LLC
Bruna Pellini, MD
Grants:
Bristol Myers Squibb Foundation
Bristol Myers Squibb
Merck/MSD
Consulting fees:
Bayer
Foundation Medicine
Guidepoint
Gilead
Regeneron
Speaker honoraria:
Amgen
AstraZeneca
Bayer
BioAscend
Boehringer Ingelheim
Bristol Myers Squibb
Catalyst
Doctaforum
Eli Lilly
Foundation Medicine
GBOT
Gilead
Grupo Pardini
Guardant Health
Illumina
MEC
Merck/MSD
Merus
MJH Life Sciences
MLI
Oncohost
Play to Know AG
Regeneron
Advisory boards or scientific steering committees:
AstraZeneca
Bayer
Boehringer Ingelheim
Bristol Myers Squibb
Catalyst
Eli Lilly
Foundation Medicine
Gilead
Illumina
Merck/MSD
Merus
OncoHost
Regeneron
06:16 – 06:32
Audio: —
[Actions]: Static screen.
[On-screen text]:
06:16 – 06:32
[On-screen text]:
Abbreviations:
HCP = healthcare professional; KEAP1 = Kelch-like ECH-associated protein 1; KRAS = Kirsten rat sarcoma; LRP1B = low-density lipoprotein receptor-related protein 1B; mPFS = median PFS; NSCLC = non-small cell lung cancer; OS = overall survival; PD-L1 = programmed death-ligand 1; PFS = progression-free survival; SMARCA4 = SWI/SNF-related, matrix-associated, actin-dependent regulator of chromatin, subfamily A, member 4; SOC = standard of care; STK11 = serine/threonine kinase 11; TMB = tumor mutational burden; TP53 = tumor protein p53.
References
- Salem ME, et al. Landscape of KRAS G12C, associated genomic alterations, and interrelation with immuno-oncology biomarkers in KRAS-mutated cancers. JCO Precis Oncol. 2022;6:e2100245.
- Xu M, et al. Unveiling the role of KRAS in tumor immune microenvironment. Biomed & Pharmacother. 2024;171:116058.
- Alsaed B, et al. Shaping the battlefield: EGFR and KRAS tumor mutations' role on the immune microenvironment and immunotherapy responses in lung cancer. Cancer Metastasis Rev. 2025;44(3):56.
- Lee JK, et al. Comprehensive pan-cancer genomic landscape of KRAS altered cancers and real-world outcomes in solid tumors. NPJ Precis Oncol. 2022;6(1):91.
- Negrao MV, et al. Oncogene-specific differences in tumor mutational burden, PD-L1 expression, and outcomes from immunotherapy in non-small cell lung cancer. J Immunother Cancer. 2021;9(8):e002891.
- Ghazali N, et al. Immunotherapy in advanced, KRAS G12C-mutant non-small-cell lung cancer: current strategies and future directions.Ther Adv Med Oncol. 2025;17:17588359251323985.
- Borg M, et al. Four decades of lung cancer: trends in comorbidities and causes of death in a nationwide Danish cohort. Eur J Cancer. 2025.218:115303.
- Wu L, et al. Pan-cancer analysis to character the clinicopathological and genomic features of KRAS-mutated patients in China. J Cancer Res Clin Oncol. 2025;151(2):94.
- He Q, et al. First-line treatments for KRAS-mutant non-small cell lung cancer: current state and future perspectives. Cancer Biol Ther. 2025;26(1):2441499.
- Mazieres J, et al. Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: results from the IMMUNOTARGET registry. Ann Oncol. 2019;30(8):1321-1328.
- Cheema PK, et al. Canadian consensus recommendations on the management of KRAS G12C-mutated NSCLC. Curr Oncol. 2023;30(7):6473-6496.
- Sheffield K, et al. Real-world outcomes with IO and chemo-IO demonstrate unmet need for 1L KRAS G12C-mutant advanced NSCLC in the US. Presented at: IASCL 2025 World Conference on Lung Cancer (WCLC); September 6-9, 2025; Barcelona, Spain. Poster 1615.
- Esfahanian N, et al. Presentation and outcomes of KRASG12C mutant non-small cell lung cancer patients with stage IV disease at diagnosis (de novo) versus at recurrence. Cancer Treat Res Commun. 2023:37:100774.
- Sabari JK, et al. Activity of adagrasib (MRTX849) in brain metastases: preclinical models and clinical data from patients with KRASG12C-mutant non-small cell lung cancer. Clin Cancer Res. 2022;28(15):3318-3328.
- Singhal A, et al. Targeting KRAS in cancer. Nat Med. 2024;30(4):969-983.
- Ferreira A, et al. Crucial role of oncogenic KRAS mutations in apoptosis and autophagy regulation: therapeutic implications. Cells. 2022;11(14):2183.
- Huang L, et al. KRAS mutation: from undruggable to druggable in cancer. Signal Transduct Target Ther. 2021;6(1):386.
- Lim TKH, et al. KRAS G12C in advanced NSCLC: prevalence, co-mutations, and testing. Lung Cancer. 2023;184:107293.
- Canon J, et al. The clinical KRAS(G12C) inhibitor AMG 510 drives anti-tumour immunity. Nature. 2019;575(7781):217-223.
- Ni T, et al. Combined inhibition of KRAS G12C and PD-1 boosts the therapeutic efficacy via conditioning of tumor microenvironment in pre-clinical humanized NSCLC mouse models. J Immunother Cancer. 2023;11(Suppl 1):A1-A1731.
- Hallin J, et al. The KRASG12C inhibitor MRTX849 provides insight toward therapeutic susceptibility of KRAS-mutant cancers in mouse models and patients. Cancer Discov. 2020;10(1):54-71.
- Brazel D, Nagasaka M. Divarasib in the evolving landscape of KRAS G12C Inhibitors for NSCLC. Target Oncol. 2024;19(3):297-301.
- Dragnev KH, et al. Safety and efficacy of olomorasib + immunotherapy in first-line treatment of patients with KRASG12C mutant advanced NSCLC: update from the LOXO-RAS-20001 trial. JCO. 2025;43(suppl).
- Fujiwara Y, et al. Efficacy and safety of olomorasib with pembrolizumab + chemotherapy as first-line treatment in patients with KRAS G12C-mutant advanced NSCLC. JCO. 2024;19(10):S41-S42.
- Sacher AG, et al. MK-1084 for KRAS G12C-mutated (mut) metastatic non–small-cell lung cancer (mNSCLC): results from KANDLELIT-001. J Clin Oncol. 2025;43(Number 16_suppl). ASCO Annual Meeting I abstract 8605.
- Garassino MC, et al. LBA65 KRYSTAL-7: efficacy and safety of adagrasib with pembrolizumab in patients with treatment-naïve, advanced non-small cell lung cancer (NSCLC) harboring a KRASG12C mutation. Ann Oncol. 2023;34:S1309-S1310.
- Li BT, Clarke JM, Felip E, et al. Sotorasib plus carboplatin and pemetrexed in KRAS G12C advanced NSCLC: Updated analysis from the international CodeBreaK 101 trial. J Clin Oncol. 2024;42(16_suppl):8512.
- ClinicalTrials.gov identifier: NCT06793215. Accessed September 11, 2025. https://clinicaltrials.gov/study/NCT06793215?cond=NSCLC
- ClinicalTrials.gov identifier: NCT06345729. Accessed September 11, 2025. https://clinicaltrials.gov/study/NCT06345729?cond=NSCLC
- ClinicalTrials.gov identifier: NCT04613596. Accessed September 11, 2025. https://clinicaltrials.gov/study/NCT04613596?cond=NSCLC
- ClinicalTrials.gov identifier: NCT06119581. Accessed September 11, 2025. https://clinicaltrials.gov/study/NCT06119581?cond=NSCLC
- ClinicalTrials.gov identifier: NCT06875310. Accessed September 11, 2025. https://clinicaltrials.gov/study/NCT06875310?cond=NSCLC
- ClinicalTrials.gov identifier: NCT05920356. Accessed September 11, 2025. https://clinicaltrials.gov/study/NCT05920356?cond=NSCLC
- ClinicalTrials.gov identifier: NCT07190248. Accessed October 6, 2025. https://clinicaltrials.gov/study/NCT07190248?cond=NSCLC
- Karimi N, Moghaddam SJ. KRAS-mutant lung cancer: Targeting molecular and immunologic pathways, therapeutic advantages and restrictions. Cells. 2023;12(5):749.
06:33 – 06:36
Audio: —
[Actions]: Lilly logo and project code animate onscreen.
[On-screen text]: V-MED-175876 © 2025 Eli Lilly and Company. All rights reserved.
1L = first-line; 2L = second-line; ALK = anaplastic lymphoma kinase; BRAF = B-rapidly accelerated fibrosarcoma; EGFR = epidermal growth factor receptor; HER2 = human epidermal growth factor receptor 2; IO = immunotherapy; KEAP1 = Kelch-like ECH-associated protein 1; KRAS = Kirsten rat sarcoma; LRP1B = low-density lipoprotein receptor-related protein 1B; MET = mesenchymal-epithelial transition; NRG1 = neuregulin 1; NSCLC = non-small cell lung cancer; NTRK = neurotrophic tyrosine receptor kinase; OS = overall survival; PD-L1 = programmed death-ligand 1; PFS = progression-free survival; RET = rearranged during transfection; ROS1 = ROS proto-oncogene 1; SMARCA4 = SWI/SNF-related, matrix-associated, actin-dependent regulator of chromatin, subfamily A, member 4; STK11 = serine/threonine kinase 11; TMB = tumor mutational burden; TME = tumor microenvironment; TP53 = tumor protein p53.
References
- Chevallier M, et al. Oncogenic driver mutations in non-small cell lung cancer: past, present and future. World J Clin Oncol. 2021;12(4):217-237.
- ACS. What is lung cancer? Last revised January 29, 2024. Accessed August 17, 2025. https://www.cancer.org/cancer/types/lung-cancer/about/what-is.html
- Acker F, et al. KRAS mutations in squamous cell carcinomas of the lung. Front Oncol. 2021;11:788084.
- Lee JK, et al. Comprehensive pan-cancer genomic landscape of KRAS altered cancers and real-world outcomes in solid tumors. NPJ Precis Oncol. 2022;6(1):91.
- Salem ME, et al. Landscape of KRASG12C, associated genomic alterations, and interrelation with immuno-oncology biomarkers in KRAS-mutated cancers. JCO Precis Oncol. 2022;6:e2100245.
- Wang X, et al. Association between smoking history and tumor mutation burden in advanced non-small cell lung cancer. Cancer Res. 2021;81(9):2566-2573.
- Xu M, et al. Unveiling the role of KRAS in tumor immune microenvironment. Biomed Pharmacother. 2024;171:116058.
- Alsaed B, et al. Shaping the battlefield: EGFR and KRAS tumor mutations' role on the immune microenvironment and immunotherapy responses in lung cancer. Cancer Metastasis Rev. 2025;44(3):56.
- He Q, et al. First-line treatments for KRAS-mutant non-small cell lung cancer: current state and future perspectives. Cancer Biol Ther. 2025;26(1):2441499.
- Cheema PK, et al. Canadian Consensus Recommendations on the management of KRAS G12C-mutated NSCLC. Curr Oncol. 2023;30(7):6473-6496.
- Wu L, et al. Pan-cancer analysis to character the clinicopathological and genomic features of KRAS-mutated patients in China. J Cancer Res Clin Oncol. 2025;151(2):94.
- Judd J, et al. Characterization of KRAS mutation subtypes in non-small cell lung cancer. Mol Cancer Ther. 2021;20(12):2577-2584.
- Negrao MV, et al. Oncogene-specific differences in tumor mutational burden, PD-L1 expression, and outcomes from immunotherapy in non-small cell lung cancer. J Immunother Cancer. 2021;9(8):e002891.
- Ghazali N, et al. Immunotherapy in advanced, KRAS G12C-mutant non-small-cell lung cancer: current strategies and future directions. Ther Adv Med Oncol. 2025;17:17588359251323985.
- Hendriks LE, et al. Non-oncogene-addicted metastatic non-small-cell lung cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2023;34(4):358-376.
- Sheffield K, et al. Real-world outcomes with IO and chemo-IO demonstrate unmet need for 1L KRAS G12C-mutant advanced NSCLC in the US. Presented at: IASCL 2025 World Conference on Lung Cancer (WCLC); September 6-9, 2025; Barcelona, Spain. Poster 1615.
- Julian C, et al. Overall survival in patients with advanced non-small cell lung cancer with KRAS G12C mutation with or without STK11 and/or KEAP1 mutations in a real-world setting. BMC Cancer. 2023;23(1):352.
- Dudnik E, et al. BRAF mutant lung cancer: programmed death ligand 1 expression, tumor mutational burden, microsatellite instability status, and response to immune check-point inhibitors. J Thorac Oncol. 2018;13(8):1128-1137.
VV-MED-175543
Please rate your satisfaction with the content on the following statements:
Very Dissatisfied
Dissatisfied
Neutral
Satisfied
Very Satisfied