You are now leaving the Lilly Medical Education website
The link you clicked on will take you to a site maintained by a third party, which is solely responsible for its content. Lilly USA, LLC does not control, influence, or endorse this site, and the opinions, claims, or comments expressed on this site should not be attributed to Lilly USA, LLC. Lilly USA, LLC is not responsible for the privacy policy of any third-party websites. We encourage you to read the privacy policy of every website you visit.
Click "Continue" to proceed or "Return" to return to Lilly Medical Education.
Communication Toolkit for Alzheimer’s Disease
Communicating Treatment & Monitoring
This page is part of a larger communication toolkit which provides general advice and best practices around communication of Alzheimer's disease (AD) in clinical practice.
See a full list of resources available on communicating a diagnosis of Alzheimer's disease.
Conversational Dynamics
The patient
Different patients have different conversational needs. Some may be keen to participate, seeking additional information proactively, while others may be apprehensive and unwilling to receive a lot of information.
Patients want great involvement in conversations around social decisions, but prefer that healthcare providers be heavily involved in medication decisions.
According to a study by Hamman et al (2011), patients with higher MMSE scores desire more involvement in decision making, while patients with lower MMSE score refrain from participation.
The Triad: Complex conversations in AD communications
The patient’s care partners play a critical role in medical conversations and patient care. Their involvement creates a triad, which can enhance communication and lead to superior comprehension.
Triadic interactions are more complex than dyadic HCP-patient conversations, and require active management to ensure that patients are not excluded from care discussions.2

MANAGING TRIADIC INTERACTIONS2
Common problems and potential solutions
There is sometimes confusion around who is to speak, and when.
Agree on rules of conduct and roles at the start of the conversation. Who talks? About what? When?
Conversations tend to become a series of dyadic interactions. The patient is initially the focus, but as conversation about treatment progresses, focus shifts to care partner.2
Explicitly articulate the goal of ensuring that the patient participates optimally in their own care decisions if they desire.
Communicating Treatment
Communicating treatments for AD
- An estimated 7.2 million Americans age 65 and older live with Alzheimer’s dementia in 2025.3 Given the impact of AD, there is an urgent need for effective therapies.6
- High quality healthcare communication has been shown to have a positive effect on patient outcomes such as treatment adherence, well-being, illness recovery and physiological reactions to diagnoses.7
- A timely and accurate diagnosis of AD is more important than ever with the availability of amyloid-targeting therapies.8,9
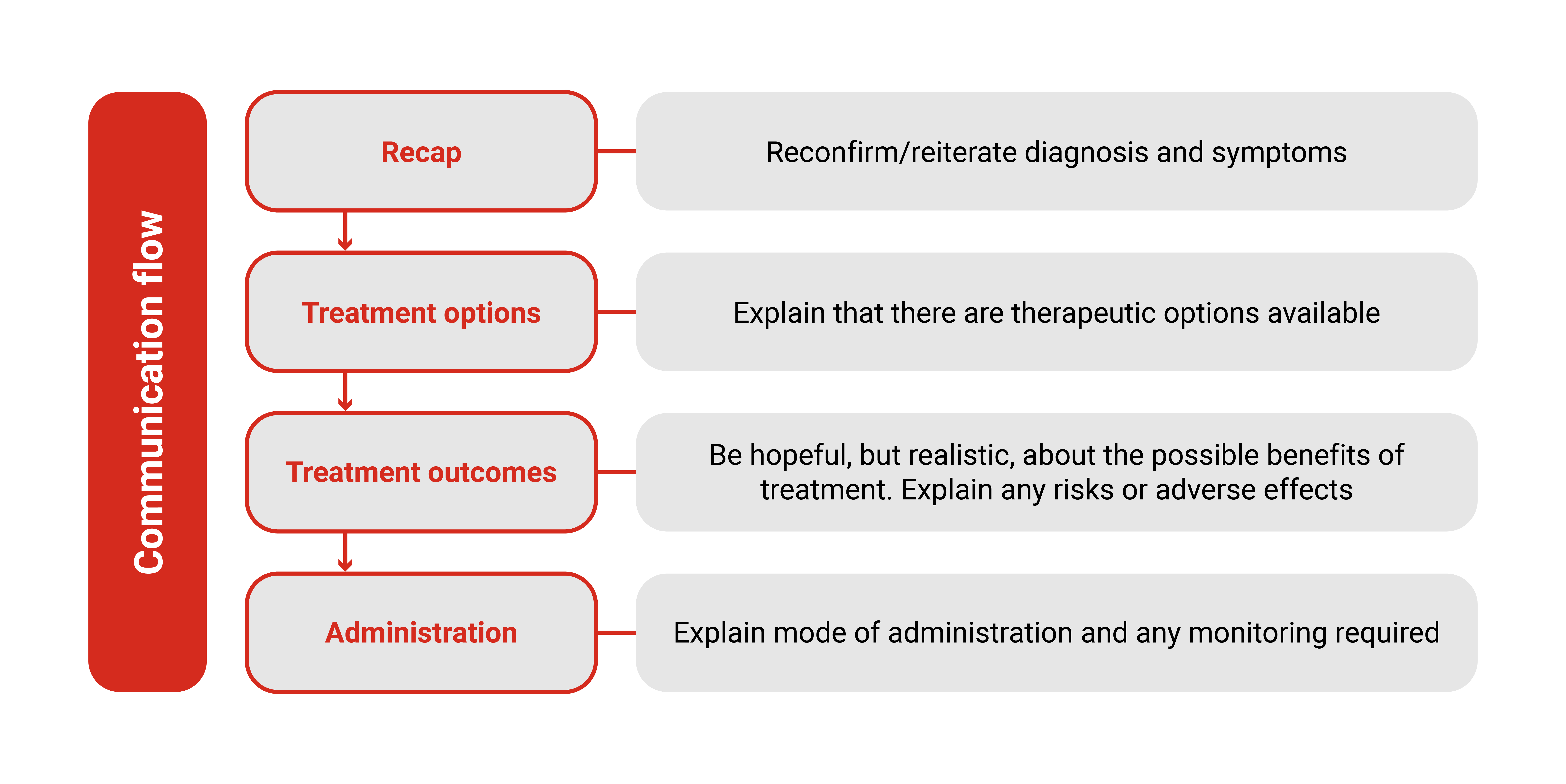
The steps are:
- Recap conversation so far around the diagnosis and symptoms;
- Explain that there are treatment options available;
- Be hopeful, but realistic about treatment outcomes by discussing possible benefits as well as any risks or side effects;
- Explain mode of administration and any monitoring required.
General Advice and Good Practices
Use strategies for nonverbal communication
80% of communication in medical and nonmedical situations occurs nonverbally, involuntarily, and outside conscious awareness, while only 20% is verbal and voluntary.5
Use patient-centric language. Patient-centered HCP–patient communication has been demonstrated to increase patient adherence to treatment, improve satisfaction with care, and decrease patient distress.4
Be concrete with treatment options and recommendations, preferably accompanying verbal information with hand-outs.
Related Resources
Downloadable PDFs
A communication support framework to guide interactions with patients and loved ones on expectations for treatment and monitoring after initation of amyloid targeting therapies.
A support communication guide to help convey important information to patients and care partners on the need for long-term monitoring.
Introspective music plays
Introspective music plays
Introspective music plays
Voiceover
We would like to thank Dr. Sharon Cohen for providing her time and expertise for this educational material.
Dr. Sharon Cohen is a full-time salaried employee of Toronto memory program and has no financial conflicts of interest.
She has lent her expertise in consulting roles, for no personal fees, to Anylam, Biogen, Bristol-Myers Squibb, Cassava Sciences, Cognivue, Cogstate, Eisai, Eli Lilly, INmune Bio, Lundbeck, Novo Nordisk, Parexel, ProMIS Neurosciences, RetiSpec and Roche.
Dr. Cohen has received research grants, which was paid to her institution only, from AbbVie, AgeneBio, Alector, Alnylam, Alzheon, Anavex, Biogen, Cassava Sciences, Eisai, Eli Lilly, GAP, Green Valley, Janssen, Novo Nordisk, RetiSpec, Roche and UCB Biopharma.
Introspective music plays
Introspective music plays
Introspective music plays
Introspective music plays
Introspective music plays
Hello. I'm Sharon Cohen.
I'm a behavioral neurologist in Toronto, Canada. And it's my pleasure to share with you how I discuss disease modifying treatments for Alzheimer's with patients. It's often a challenge because not all physicians are used to prescribing disease modifying therapies in this therapeutic area. What I tell patients is that we now have an opportunity to slow their disease.
Introspective music plays
So, Mr. Smith, you're still driving, you're still working. I want to keep you that way as long as possible.
We now have a treatment given intravenously that targets the underlying brain changes of Alzheimer's, something called amyloid. And if we clear amyloid, we can slow down the disease.
We don't cure it, we don't reverse it.
But keeping you at a mild stage longer is really worthwhile. Would you agree?
That's the nature of the conversation that I have. And then I talk about the risks,
and the main risk is something called ARIA. And what I say to patients is….
some people on these amyloid clearing medicines will experience something we call ARIA. And this comes about because blood vessels become a little bit leaky and there can be spots of bleeding or areas of swelling in the brain.
And although that sounds very dramatic and scary, most of the time, there are no symptoms.
Fortunately, we can monitor with MRI scans and see if this is occurring, this thing we call ARIA, and if it is, then we may hold the treatment until ARIA clears. It generally clears over a few months and most of the time, if there are symptoms,….
….these symptoms are mild or moderate, rarely serious or severe. But nonetheless, we take this seriously and we will monitor to keep you safe.
That usually alleviates a lot of fears, and then depending on the nature of a patient or family's questions, we would go from there.
Introspective music plays
Introspective music plays
Communicating Treatment Options after a Diagnosis of Alzheimer's Disease
Dr. Sharon Cohen provides recommendations on how to introduce amyloid-targeting therapies to patients after a diagnosis of Alzheimer's disease.
Introspective music plays
Introspective music plays
Introspective music plays
Voiceover:
We would like to thank Dr. Richard Perry for providing his time and expertise for this educational material.
Dr. Richard Perry has performed advisory and educational work for Lilly, Roche, Biogen and MSD
Introspective music plays
Introspective music plays
Introspective music plays
Introspective music plays
I thought we might just start just by recapping what we discussed last time….
….and then having a think about what our options are, and particularly about treatment options. So when you came last time, we'd done some investigations and the investigations confirmed that this memory difficulty is likely to be the early stages of Alzheimer's disease.
And we’d started one medication to help with your symptoms. And it's good to hear that you're steady on that now and that's going all right. Today, I just wanted to have a chat about the options for a different kind of treatment. So, to give you the background on this, I think it's important that we just talk a little bit about what the medications try to do and how they work.
So when people have conditions like Alzheimer's disease, there's usually a process underlying it. And one of the key features of Alzheimer's disease is there's a build up of proteins in the brain. And one of the important ones is amyloid, and that's a protein that builds up very early in this process.
When people have been trying to develop medications to treat Alzheimer's disease, one of the targets has been removing amyloid protein. So there are drugs available that we know are quite effective at removing amyloid protein. And the hope is that by doing that early enough, we can slow down the condition a little. They're not medications that are going to reverse things and make things like they used to be, and they're probably not going to halt things entirely.
But if they slow the process down, then the benefit of that is that people can keep doing things for longer. So at the moment, the memory difficulties, you've got a mild and you're doing all those activities that we spoke about earlier. And the idea is that if we try this medication early enough, then we can slow that down and keep you doing all that for longer.
Introspective music plays
Introspective music plays
Communicating Amyloid Pathology and Treatment Options to Patients
Dr. Richard Perry provides recommendations on how to explain amyloid pathology and introduce amyloid-targeting therapies as a possible treatment option to patients.
Introspective music plays
span>Introspective music plays
span>Introspective music plays
(Voiceover) We would like to thank Dr. Anna Burke for providing her time and expertise for this educational material.
Dr. Anna Burke is a full-time salaried employee of Dignity Health, and has the following disclosures:
She has lent expertise in consulting roles, for no personal fee, to Eli Lilly, Roche and Eisai.
Dr. Anna Burke has received research grants, paid to her institution only, from Eli Lilly, Biogen, Alector, AbbVie, Cognito, Roche, and Janssen.
span>Introspective music plays
span>Introspective music plays
span>Introspective music plays
span>Introspective music plays
Anna Burke:
Now, the medication that you're on right now helps your brain cells communicate with each other a little bit better. But it really doesn't do much as far as the damage that's occurring to your brain.
Some of the new medications that have become available actually attack the illness itself by minimizing some of the damage that's occurring to the brain.
Anna Burke:
Now, these medications can be helpful in slowing the disease process, but they do come with some risks. As we remove amyloid from the brain, we're trying to remove it from in between brain cells where it causes much of the damage. But unfortunately, amyloid also likes to build up inside blood vessel walls in the brain. And as we remove it from the brain, we're removing it everywhere, including from those blood vessel walls. That means sometimes we can open up some pores in those blood vessel walls, and they can leak. They can leak a little bit of fluid, or they can leak a little bit of blood, causing something called ARIA phenomenon. Luckily, that ARIA phenomenon in most cases is not something that presents with clinical symptoms. So most people don't even know that they have it.
Anna Burke:
And it is something that we can pick up on, on imaging, like an MRI of the brain.
Anna Burke:
That means that if you do undergo this type of treatment, we would need to very closely monitor you with those brain scans on a regular basis. Another thing that we would need to check is your genetic status, because we do know that there are certain individuals that are more prone to developing ARIA, and those are the individuals that have a certain genetic variant called the ApoE4 allele.
Anna Burke:
I would recommend that we do some additional genetic testing….
Anna Burke:
….just to determine what your risk of developing ARIA with this new treatment would be.
Introspective music plays
Introspective music plays
Providing Patients and Care Partners with Necessary Treatment Information
Dr. Anna Burke provides recommendations on how to discuss benefits and risks with patients considering amyloid-targeting therapies.
Introspective music plays
Introspective music plays
(Voiceover) We would like to thank Dr. Reeta Achari for providing her time and expertise for this educational material.
Dr. Reeta Achari has done advisory and educational work for Eli Lilly and Company.
Introspective music plays
Introspective music plays
Introspective music plays
Introspective music plays
Reeta Achari:
So the first thing to know is that memory disorders, memory impairment and memory loss are not a normal part of aging.
Reeta Achari:
And we shouldn't think of it that way. And it's extremely important to establish a precise and accurate diagnosis of the kind of memory disorder. We have ways now to determine if the type of memory disorder you're having is Alzheimer's disease or other types of memory disorders. With Alzheimer's disease, with wonderful new research and all the activity that's been going on, we now have treatments and those treatments are available and effective when used early. So, being timely in making this diagnosis properly is really important. In terms of using these treatments they require from the patient a commitment. They're not simple as taking a pill. They're slightly more complicated, but the brain is a more complicated organ. What I want all of my patients to know and what caregivers also should know, is that this requires a degree of time. So there will be infusions. So intravenous medications at this point, they may change later on in the future, that will be given at regular intervals.
Reeta Achari:
We've talked about the benefit.
Reeta Achari:
The benefit is that it will slow down the progression of the illness. What are the side effects and the risk factors associated with these types of therapies?
One may be an infusion reaction, so when the medication is infused, you may have a transient and feeling of unease, chills, some flushing, which will go away. You might be allergic to the medication. And as we know, if you're allergic to anything, you are no longer to have that medication.
Reeta Achari:
All in all, there is a nice algorithm now to help us take care of patients who will be eligible for these therapies
Reeta Achari:
and this is a very bright spot in the understanding of a disease that has been difficult for us to deal with for many decades now, and hopefully, hopefully will lead to even more treatments.
Introspective music plays
Introspective music plays
Treatment Expectations when Starting ATTs for Patients and Care Partners
Dr. Reeta Achari provides recommendations on how to discuss treatment expectations when starting patients on amyloid-targeting therapies.
0:15-0:45
Ana Franceschi: From a multidisciplinary perspective, I cannot emphasize how important communication is to us as radiologists. And this goes both ways. When interpreting cases, you know, having a robust clinical history and really the reason for the scan is extremely important. And then also in the other direction, communicating pertinent results, especially in the context of ARIA findings, directly to the ordering neurologists and ordering providers is extremely helpful.
0:45-1:11
Ana Franceschi: So, in the context of dementia imaging, it's really important to have as detailed clinical history as possible for an appropriate interpretation or clinically relevant interpretation. This typically includes patients' key symptoms, preferably results of cognitive testing, such as MOCA and MMSE scores, and any additional data that might be pertinent to put the findings into clinical context.
1:11-1:45
Ana Franceschi: It's very important for the clinicians, the neurologists, to keep in mind that many different pathologies can look very similar in imaging. And in this context, clinical history is key. This goes for both appropriately identifying ARIA on an MRI scan and differentiating it from potential mimics. But it also goes towards the context of an accurate diagnosis of an underlying neurodegenerative disease, both from an FDG PET standpoint and also from a structural imaging standpoint.
1:45-2:35
Ana Franceschi: When interpreting dementia imaging studies, it is very important to effectively communicate pertinent results to the referring clinicians. A few things to keep in mind from an ARIA assessment standpoint is that ARIA is inherently an imaging-based phenomenon. And about 90% of all cases are asymptomatic. So, if patients are coming in for a routine screening scan, there may be a delay in recognition of the diagnosis by the neurologist or the referring clinicians. So especially in cases where the report may impact clinical decision and treatment plans, such as in moderate or severe ARIA cases, it is very important to initiate a physician to physician communication and document this in your report.
2:35-3:02
Ana Franceschi: In my experience, neurologists and other physicians find it very helpful to hear directly from the radiologist when there are some pertinent positive findings. These therapies are still new, and we're just learning about the clinical impact and the clinical frequency of them. So typically, I initiate a phone call for all ARIA cases that I see on imaging, regardless of severity.
3:02-3:30
Ana Franceschi: From a communication standpoint, it's also very important to highlight the multidisciplinary conferences that are present in most institutions. We have a dementia board where we discuss our diagnostically challenging cases, both from a clinical and from an imaging standpoint. But we also discuss our patients on anti-amyloid therapies and discuss next steps and management decisions for these patients.
Enhancing Alzheimer’s Disease Imaging Through Effective Interdisciplinary Communication
In this video, Dr. Francheschi emphasizes the importance of effective interdisciplinary communication in dementia imaging and ARIA assessment.
0:15-0:39
Richard Perry: With these kinds of treatments, we often start off with a sort of prescriber and the people who are doing all the diagnostic testing and doing the scans. But going earlier in that journey and thinking about the primary care physicians, what do they need? What are their concerns? You know, what is the biggest barrier for them in terms of seeing people and identifying and referring them on?
0:40-1:41
Pascual Sanchez Juan: Well, the role of general practitioners is going to be essential. They are the first step. Because we need really to apply this treatment early, we need to get the patients as soon as possible. So, they are going to play a very, very important role in detecting the first signs. So, they need more aware of the first symptoms of the disease. They need more tools in order to be more specific in the diagnosis. And probably they need more time because sometimes general practitioners do not have a lot of time. So, it would be important that for these kinds of patients they save more time, and they have some help, for example, of the nurse that helped them to do some of the neuropsychological testing. So, if plasma biomarkers come to the clinic, which is something that we expect that it will happen soon, this could be a very important tool that can help us to better select the patients that are and that goes to the specialist for assessing the treatment.
1:42-2:59
Monica Parker Willis: I think as a team, you have to work together to manage a person's usually complex problem because it takes more than one specialist to usually manage those things. You need to have, develop a system for that communication. And if it's in a singular health system, it may be made easier because we have an electronic health record. But more commonly, there needs to be one to one physician to physician direct communication. So, if people are undergoing specialty therapies, whether it's a cancer chemotherapy or a cognitive monoclonal antibody or ulcerative colitis or Crohn's disease, there needs to be some communication between that primary care doctor and that subspecialist. There needs to be an understanding of this is what I do, this is what you do, tell me how you want to relate. Most doctors do that within their systems. But that doesn't mean that if I send you to the specialist, I'm just sending you over there without giving him or her any kind of background. So, provider to provider, this is what I've done, this is what I've found. I can't do anything more with this. Can you help me? I'm referring him. That's a proper handoff to me.
2:59-3:33
Laura Bonnani: Yeah. So, I think that during monitoring of the treatments for Alzheimer's disease and in general for Alzheimer's disease independently of the treatment, it's important to have a multidisciplinary team where neurologists, primary care practitioner, the radiologist, the nuclear medicine specialists can talk together and discuss the cases. As happens already for other specialties like oncology. So, I think it's very important, the confrontation, the comparison of opinions between different specialists.
Multidisciplinary Approaches to Alzheimer's Disease Management
Explore interdisciplinary communication from a Neurologist and PCP perspective, providing key insights into communicating patient hand offs and essential follow up information.
Chapter 1: Communicating Treatment Options and Shared Decision-Making
[00:00:00 – 00:16:16] Ambient Travel Background Music performed by Adobe Stock plays
[00:16:17 – 00:26:01] Voiceover: Amyloid-targeting therapies (ATTs) are novel therapeutics requiring clear communication for patient understanding.
[00:26:02 – 00:36:61] Voiceover: Based on expert insights, this is a suggested communication flow for discussing Amyloid-Targeting Therapy with your patients and their care partner.
[00:36:62 – 00:46:78] Voiceover: This series of educational videos provide advice on techniques using this communication approach together with best practices disclosures by our panel of top thought leaders.
[00:46:79 – 00:55:99] Voiceover: This video series aims to support healthcare providers in communicating ATTs as a novel therapy option.
[00:56:00 – 00:59:52] Ambient Travel Background Music performed by Adobe Stock plays
[00:59:53 – 01:09:57] Voiceover: In this video, we will discuss effective communication strategies for establishing the basis for treatment discussion and shared decision-making in the Alzheimer's disease treatment journey.
[01:09:58 – 01:15:08] Ambient Travel Background Music performed by Adobe Stock plays
[01:15:09 – 01:26:70] Voiceover: Patients with early symptomatic Alzheimer's disease can understand and participate in treatment discussions but struggle to make optimal decisions in risky and ambiguous situations.
[01:26:71 – 01:38:52] Voiceover: Different patients require different communication approaches. Tailoring information to their preferences helps establish a foundation for discussing treatment options.
[01:38:53 – 01:51:05] Voiceover: Effective communication is crucial for Alzheimer's disease diagnosis and treatment discussions. Let's look at some conversations shared by our experts:
[01:51:06 – 01:56:44] Dr. Richard Perry: I thought we might just start just by recapping what we discussed last time....
[01:56:45 – 02:04:24] Dr. Richard Perry: ....and then having a think about what our options are, and particularly about treatment options.
[02:04:24 – 02:25:20] Dr. Richard Perry: So when you came last time, we'd done some investigations, and the investigations confirmed that this memory difficulty is likely to be the early stages of Alzheimer's disease. And we had started one medication to help with your symptoms. And it's good to hear that you're steady on that now.
[02:25:21 – 02:31:38] Ambient Travel Background Music performed by Adobe Stock plays
[02:31:39 – 02:38:27] Dr. Anna Burke: Now, we do have some new treatments that are available in addition to the medication that you're already on.
[02:38:28 – 02:42:38] Dr. Anna Burke: And, and I think it's important for us to discuss some of your options.
[02:42:39 – 03:12:10] Dr. Anna Burke: The medication that you were already taking is one that helps your brain cells communicate a little bit better, but it really doesn't do much in terms of damage that's occurring to your brain. Some of the new medications that have recently become available actually do address the underlying damage that occurs to the brain. So these are some of these disease modifying therapies or anti amyloid monoclonal antibodies.
[03:12:11 – 03:18:71] Ambient Travel Background Music performed by Adobe Stock plays
[03:18:72 – 03:31:09] Voiceover: Shared decision-making, the collaborative process in which the physician works together with the patient to reach a joint decision about care, may be a method that is currently used in your clinical practice.
[03:31:10 – 03:40:46] Voiceover: This has several benefits, and is preferred by patients with dementia, cognitive impairment or Alzheimer's disease.
[03:40:47 – 03:53:26] Voiceover: Commonly the patient is accompanied by a care partner. This is preferred for enhanced communication, comprehension and recall. However, it is important to keep the patient as the priority.
[03:53:27 – 04:01:79] Voiceover: These are the key takeaways on communicating treatment options and shared decision-making.
[04:01:80 – 04:06:80] Ambient Travel Background Music performed by Adobe Stock plays
[04:06:81 – 04:11:99] Ambient Travel Background Music performed by Adobe Stock plays
Communicating Treatment Options and Shared Decision-Making
Discover communication practices with patients and care partners about amyloid targeting therapies, including setting the foundation, treatment options, and shared decision-making.
Voiceover Narration:
00:16:17 – 00:26:41:
“Based on expert insights, this is a suggested communication flow for discussing amyloid targeting therapy with your patients and their care partner.”
00:26:42 – 00:36:75:
“This series of educational videos provide advice on techniques using this communication approach together with best practices disclosures by our panel of top thought leaders.”
00:36:76 – 00:45:91:
“This video series aims to support healthcare providers in communicating ATTs as a novel therapy option.”
00:49:57 – 01:00:49:
“In video 2 of this video series, we will discuss effective strategies for communicating the pathology of Alzheimer's disease,….”
01:00:50 – 01:07:39:
“…. the mechanism of action of amyloid targeting therapies with your patient and their care partner, as well as techniques on how to improve recall and patient understanding.”
01:07:40 – 01:16:81:
“Let's listen to best practices from our expert on explaining amyloid pathology and the mechanism of action of ATT.”
Dr. Anna Burke:
01:16:82 – 01:21:31:
“Some of the new medications that have become available….”
01:21:32 – 01:28:00:
“….actually attack the illness itself by minimizing some of the damage that's occurring to the brain.”
01:28:01 – 01:30:22:
“The way that they work is by removing….”
01:30:23 – 01:39:22:
“….The way that they work is by removing a protein that builds up inside your brain called amyloid.”
01:39:23 – 01:39:96:
“We believe that that amyloid is involved in the cascade that leads to brain cell death,….”
01:39:97 – 01:53:97:
“….and that by removing that amyloid we may be able to minimize some of the damage and help slow the disease process.”
Voiceover Narration (continued):
01:59:66 – 02:11:58:
“There are different approaches to improve conversation, recall and patient understanding. The amount of information presented influences recall.”
02:11:59 – 02:22:34:
“Additionally, information shared at the start or end of a conversation is more likely to be remembered, especially when it is specific.”
02:22:35 – 02:29:05:
“Visual aids can influence both attention, comprehension and recall.”
02:29:06 – 02:36:75:
“Take a moment to ensure the patient understands the information provided.”
02:36:76 – 02:52:07:
“Providing additional resources, like written summaries of diagnoses, plans, and relevant information, can improve understanding and recall for patients and care partners.”
Communicating Amyloid Pathology and Improving Patient Understanding
Discover communication practices with patients and care partners about amyloid targeting therapies, including amyloid pathology, MOA, and ensuring understanding.
Chapter 3: Communicating Benefits and Risks of Amyloid Targeting Therapy
Time Stamp: 00:00:00 – 00:15:78 Ambient Travel Background Music performed by Adobe Stock plays
Time Stamp: 00:15:79 – 00:26:56 Voiceover: Based on expert insights, this is a suggested communication flow for discussing amyloid targeting therapy with your patients and their care partner.
Time Stamp: 00:26:57 – 00:36:78 Voiceover: This series of educational videos provide advice on techniques using this communication approach together with best practices disclosures by our panel of top thought leaders.
Time Stamp: 00:36:79 – 00:45:67 Voiceover: This video series aims to support healthcare providers in communicating ATTs as a novel therapy option.
Time Stamp: 00:45:68 – 00:49:37 Ambient Travel Background Music performed by Adobe Stock plays
Time Stamp: 00:49:38 – 01:00:70 Voiceover: In video 3 of this video series, we will discuss effective strategies to convey the benefits and side-effects of ATTs and how you can communicate about risks and uncertainty towards your patients.
Time Stamp: 01:00:71 – 01:05:79 Ambient Travel Background Music performed by Adobe Stock plays
Time Stamp: 01:05:80 – 01:10:76 Voiceover: Let's listen to best practices from the experts.
Time Stamp: 01:12:96 – 01:29:01 Dr. Reeta Achari: ….help slow down the progression of this illness, allowing you to stay functional, to stay, doing and doing the things that you are doing now.
Time Stamp: 01:29:02 – 01:29:27 Dr. Reeta Achari: It allows you to be you longer.
Time Stamp: 01:29:28 – 01:37:27 Dr. Richard Perry: I thought it'd be useful just to talk a little bit about some of the side-effects of medications….
Time Stamp: 01:37:27 – 01:46:16 Dr. Richard Perry: ….because it's important to balance what sort of benefit we're expecting against what might be the side-effects.
Time Stamp: 01:46:17 – 01:48:82 Dr. Richard Perry: In terms of the potential side-effects, most people don't get side-effects with medication.
Time Stamp: 01:48:83 – 01:54:60 Ambient Travel Background Music performed by Adobe Stock plays
Time Stamp: 01:54:61 – 01:57:70 Dr. Anna Burke: Amyloid….
Time Stamp: 01:57:71 – 02:15:47 Dr. Anna Burke: ….likes to build up in between brain cells where we believe it does most of the damage. But unfortunately, amyloid also builds up inside blood vessel walls in the brain.
Time Stamp: 02:15:48 – 02:31:91 Dr. Anna Burke: And as we’re dissolving that amyloid in the brain, we can't selectively dissolve it from just in between brain cells; we're dissolving it everywhere, which means sometimes we can open up pores inside those blood vessel walls, and those pores may leak a little bit of fluid or a little bit of blood, causing something called ARIA phenomenon.
Time Stamp: 02:31:92 – 02:48:88 Dr. Richard Perry: Sometimes people can get symptoms, headaches, dizziness, occasionally they can be a bit muddled or have speech problems, but that's quite rare. If we were to have those kind of symptoms, we'd do extra scans to make sure there are no changes on the scans …
Time Stamp: 02:48:89 – 03:20:42 Dr. Richard Perry: …and we would stop the medication and wait until everything settles down. And it's also important to understand that in very rare situations there may be more severe symptoms where the leakage of blood vessels is bigger and can cause difficulties with speech, stroke-like symptoms, or even possibly disability or death. But I think that's a very rare occurrence and we can go through the exact figures for that.
Time Stamp: 03:20:43 – 03:22:48 Dr. Anna Burke: We know that certain individuals are more prone ….
Time Stamp: 03:22:49 – 03:25:06 Dr. Anna Burke: ….to developing this ARIA phenomenon than others. In particular, individuals who carry a certain genetic variant called the APOE4 allele are more prone to developing ARIA.
Time Stamp: 03:35:81 – 03:42:02 Ambient Travel Background Music performed by Adobe Stock plays
Time Stamp: 03:42:03 – 03:51:35 Voiceover: Risk perception varies between objective facts and personal feelings, shaped by context, perceived likelihood, and severity.
Time Stamp: 03:51:36 – 03:57:12 Voiceover: Remember to avoid only verbal descriptions as these can be interpreted very differently between people.
Time Stamp: 03:57:13 – 04:06:01 Voiceover: Keep in mind that many patients have low numeracy skills. Use pictographs to communicate risk and benefit information.
Time Stamp: 04:06:02 – 04:14:44 Ambient Travel Background Music performed by Adobe Stock plays
Time Stamp: 04:14:45 – 04:19:33 Ambient Travel Background Music performed by Adobe Stock plays
Time Stamp: 04:19:34 – 04:24:98 Ambient Travel Background Music performed by Adobe Stock plays
Communicating Benefits and Risks of Amyloid Targeting Therapies
Discover communication practices with patients and care partners about amyloid targeting therapies, including benefits and risks, such as ARIA, and uncertainty.
Chapter 4: Communicating Administration and Treatment Management with Realistic Expectations
Time Stamp: 00:00:00 – 00:00:96 Ambient Travel Background Music performed by Adobe Stock plays
Time Stamp: 00:00:97 – 00:02:32 Ambient Travel Background Music performed by Adobe Stock plays
Time Stamp: 00:02:33 – 00:03:07 Ambient Travel Background Music performed by Adobe Stock plays
Time Stamp: 00:03:08 – 00:09:80 Ambient Travel Background Music performed by Adobe Stock plays
Time Stamp: 00:09:81 – 00:12:78 Ambient Travel Background Music performed by Adobe Stock plays
Time Stamp: 00:12:79 – 00:15:78 Ambient Travel Background Music performed by Adobe Stock plays
Time Stamp: 00:15:79 – 00:26:56 Voiceover: Based on expert insights, this is a suggested communication flow for discussing amyloid targeting therapy with your patients and their care partner.
Time Stamp: 00:26:57 – 00:36:78 Voiceover: This series of educational videos provide advice on techniques using this communication approach together with best practices disclosures by our panel of top thought leaders.
Time Stamp: 00:36:79 – 00:45:67 Voiceover: This video series aims to support healthcare providers in communicating ATTs as a novel therapy option.
Time Stamp: 00:45:68 – 00:49:37 Ambient Travel Background Music performed by Adobe Stock plays
Time Stamp: 00:49:38 – 01:00:70 Voiceover: In this video, we will discuss effective communication of realistic treatment expectations, practical aspects of ATT administration, and monitoring and management of adverse events (AEs).
Time Stamp: 01:00:71 – 01:05:79 Ambient Travel Background Music performed by Adobe Stock plays
Time Stamp: 01:05:80 – 01:10:59 Voiceover: Let's listen to best practices from the experts.
Time Stamp: 01:10:60 – 01:12:95 Dr. Richard Perry: What's important to realize….
Time Stamp: 01:12:96 – 01:19:49 Dr. Richard Perry: ….is this isn't a medication that's a cure. It's not going to change everything back to how it was….
Time Stamp: 01:19:50 – 01:25:81 Dr. Richard Perry: ….and it's not really realistic for us to expect it to completely halt things.
Time Stamp: 01:25:82 – 01:34:82 Dr. Richard Perry: But what we're looking for is that it slows things down. And what that means is that you can keep doing what you're doing for longer.
Time Stamp: 01:34:83 – 01:41:37 Ambient Travel Background Music performed by Adobe Stock plays
Time Stamp: 01:41:38 – 01:49:46 Dr. Reeta Achari: They are not simple as taking a pill, they are slightly more complicated. But the brain is a more complicated organ.
Time Stamp: 01:49:47 – 01:57:78 Dr. Reeta Achari: The treatment process requires time and commitment from the patient and caregivers.
Time Stamp: 01:57:79 – 02:06:92 Dr. Reeta Achari: The treatments require, at this time intravenous infusions, which are to be given periodically.
Time Stamp: 02:06:93 – 02:12:98 Ambient Travel Background Music performed by Adobe Stock plays
Time Stamp: 02:12:99 – 02:16:31 Dr. Reeta Achari: One may be an infusion reaction.
Time Stamp: 02:16:32 – 02:18:12 Dr. Reeta Achari: So when the medication is infused,…
Time Stamp: 02:18:13 – 02:34:44 Dr. Reeta Achari: …you may have a transient feeling of unease, chills, some flushing, which will go away. You might be allergic to the medication. And as we know, if you're allergic to anything, you are no longer to have that medication.
Time Stamp: 02:34:45 – 02:42:03 Dr. Anna Burke: Now luckily, most people who experience this ARIA phenomenon do not have any clinical symptoms;….
Time Stamp: 02:42:04 – 02:49:78 Dr. Anna Burke: ….and luckily, we are able to catch that ARIA with imaging.
Time Stamp: 02:49:79 – 03:02:33 Dr. Anna Burke: So with scans of the brain like MRI scans. That means that if you do undergo this type of treatment, we would need to very closely monitor you with those brain scans on a regular basis.
Time Stamp: 03:02:34 – 03:06:00 Dr. Reeta Achari: Sometimes the brain swelling or…
Time Stamp: 03:06:01 – 03:45:15 Dr. Reeta Achari: …brain bleeding, small amounts again, can cause symptoms and those symptoms can be variable, everything from a headache to mild confusion or disorientation, dizziness. You may have difficulty speaking, so they may present with stroke like symptoms. And in those situations, again, an MRI is done to determine what is going on. And then from there, determining depending on the findings, further continuation or maybe suspension of therapy and in some cases, discontinuation of the therapy may be needed.
Time Stamp: 03:45:16 – 03:53:13 Ambient Travel Background Music performed by Adobe Stock plays
Time Stamp: 03:53:14 – 03:58:57 Ambient Travel Background Music performed by Adobe Stock plays
Time Stamp: 03:58:57 – 04:04:20 Ambient Travel Background Music performed by Adobe Stock plays
Communicating Administration and Treatment Management with Realistic Expectations
Discover communication practices with patients and care partners about amyloid targeting therapies, including realistic expectations, administration, and adverse event management.
Voiceover Narration:
00:00:14 – 00:00:30:
“Patient eligibility status for Novel ATT Therapeutics requires clear and comprehensive communication between HCPS and patients. In this educational video series, you will explore key aspects of the eligibility conversation in five common clinical scenarios.”
00:00:30 – 00:00:35:
“In this first video, we look at 2 cases”
00:00:35 – 00:00:45:
“when the patient has early symptomatic AD with confirmed amyloid positivity and when the patient has moderate or severe AD but is interested in ATTs.”
Dr. Laura Bonanni:
00:00:45 – 00:01:35:
“So this is a very important question how to deal with the possible eligibility or non eligibility of patients.
So if it's a patient's eligible for ATT I will definitely tell that there is an option, an opportunity for a disease modifying treatment.
Of course it is important to underline that it is not like panacea or something that will remove all the symptoms of the disease or can get back the brain as it was before the development of neurogenic conditions and there is some adverse event.
But still it's a nice option and new opportunity to treat the patients.”
Dr. Anna Burke:
00:01:35 – 00:02:11:
“These can be very difficult discussions.
Many patients who come in and are interested in ATTs are very hopeful.
They have heard about these medications and sometimes they have misconceptions about what these medications can do.
Sometimes, unfortunately, they think that these are going to be therapies that will reverse their symptoms or stop the disease in its tracks.
We do have to have realistic expectations that are set in those discussions.”
Dr. Richard Perry:
00:02:18 – 00:03:14:
“The difficulty is always talking to a patient who might not be eligible, and often that's because their Alzheimer's disease has progressed to the situation where they've got a moderately or severe stage of Alzheimer's disease.
And for those patients, often they or their families would be very keen to look at these new therapies, but it might be that those new therapies are not the right medication for them and not the right medication for them really means that we don't have evidence that those medications work for people with their difficulties and that they might be exposed to the side effects.
So for people, for instance, earlier on, we've got evidence that there's benefit and we can balance that against the risks.
If you've only got risks and no evidence of benefit, then you're exposing somebody to potential side effects for drug that might not help them.”
Dr. Pascual Sanchez-Juan:
00:03:14 – 00:04:07:
“Unfortunately, we do not have that many therapeutic options, pharmacological options.
So changing in habits and it's very important.
So we communicate a list of healthy habits for the brain that they should start.
And so this is really essential and we do have a nurse that is dedicated to follow up with all these recommendations about exercise, sleep and food and cognitive stimulations.
And this is an essential part and also this needs the involvement of the family.
So this is something again that we have to discuss with the family and we need help from the family to carry on with that.”
Voiceover Narration (continued):
00:04:12 – 00:04:32:
“In this video, we explored one way to communicate ATT eligibility to patients with mild AD with confirmed amyloid positivity and patients with moderate or severe AD.
In Video 2, we will deep dive into communicating eligibility status in three other common clinical scenarios.”
Communicating Eligibility Status for Amyloid Targeting Therapies to Patients - Early Symptomatic AD, Moderate/Severe AD
Explore communicating treatment eligibility to patients when considering amyloid targeting therapies, focusing on early symptomatic and moderate/severe stages of Alzheimer's disease.
References
- Hamann, J., Bronner, K., Margull, J., Mendel, R., Diehl-Schmid, J., Bühner, M., Klein, R., Schneider, A., Kurz, A. and Perneczky, R. (2011), Patient Participation in Medical and Social Decisions in Alzheimer's Disease. J Am Geriatr Soc. 59: 2045-2052. https://doi.org/10.1111/j.1532-5415.2011.03661.x
- Karnieli-Miller O, Werner P, Aharon-Peretz J, Sinoff G, Eidelman S. Expectations, experiences, and tensions in the memory clinic: the process of diagnosis disclosure of dementia within a triad. Int Psychogeriatr. 2012;24(11):1756-1770. doi:10.1017/S1041610212000841
- 2025 Alzheimer's disease facts and figures. Alzheimer's Dement. 2025 Apr 29;21(4):e70235. doi: 10.1002/alz.70235.
- Stubbe DE. Alleviating Anxiety: Optimizing Communication With the Anxious Patient. Focus (Am Psychiatr Publ). 2017;15(2):182-184. doi:10.1176/appi.focus.20170001
- Rita Gorawara-Bhat, Mary Ann Cook, Greg A Sachs, Nonverbal communication in doctor–elderly patient transactions (NDEPT): Development of a tool, Patient Education and Counseling, Volume 66, Issue 2, 2007, Pages 223-234, ISSN 0738-3991, https://doi.org/10.1016/j.pec.2006.12.005.
- López-Antón, R. (2024). Recent Advances in Alzheimer’s Disease Research: From Biomarkers to Therapeutic Frontiers. Biomedicines, 12(12), 2816. https://doi.org/10.3390/biomedicines12122816
- Dooley J, Bailey C, McCabe R. Communication in healthcare interactions in dementia: a systematic review of observational studies. International Psychogeriatrics. 2015;27(8):1277-1300. doi:10.1017/S1041610214002890
- Porsteinsson AP, Isaacson RS, Knox S, Sabbagh MN, Rubino I. Diagnosis of Early Alzheimer's Disease: Clinical Practice in 2021. J Prev Alzheimers Dis. 2021;8(3):371-386. doi:10.14283/jpad.2021.23
- Pemberton HG, Collij LE, Heeman F, et al. Quantification of amyloid PET for future clinical use: a state-of-the-art review. Eur J Nucl Med Mol Imaging. 2022;49(10):3508-3528. doi:10.1007/s00259-022-05784-y
MMAT-06866
Please rate your satisfaction with the content on the following statements:
Very Dissatisfied
Dissatisfied
Neutral
Satisfied
Very Satisfied