Hello, I'm Dr. Deborah Bade-Horn, medical director at the UT Center for Obesity Medicine and Metabolic Performance. Thank you for joining me today to talk about the role of obesity care in your daily practice.
Here are my conflicts of interest.
And where I'd love to start is, what things do you feel most comfortable discussing with your patients already when it comes to obesity care? Are you most comfortable thinking about genetic and biological factors? Psychological factors like weight bias and stigma? Maybe you feel more comfortable talking about environmental cues that affect someone's obesity? Or perhaps, I think many of us do feel comfortable talking about psychological and behavioural factors like physical activity and sleep. For those that you might not feel as comfortable with, let's think about the things that contribute to obesity as a multifactorial disease. Here you'll see those areas in sort of four pillars and a breakdown of some of the things that fall under those pillars. So, perhaps mental health and stress are things you commonly talk to your patients about when it comes to their obesity. Or maybe you're more comfortable talking about support systems and environmental and social factors or their access to obesity treatments and what you can provide in the care for them. Remember we have two others, biological factors that I mentioned before, that aren't just genetics and epigenetics, but also include hormones and metabolism, which we're going to get into, as well as lifestyle and behavioural factors like sleep and quality and duration of that sleep or someone's physical activity level. Let's keep these four pillars in mind as we think about obesity and think about how we might share and treat our patients.
Let's start with a patient that probably resembles a patient that you see in your clinic every day. This is Roger. He's someone that in this case we would have seen about three months ago and recognized together with him that he was struggling with obesity. You can see here that at that initial visit he had a BMI in the class one range of 34.5. And at that initial visit we made some decisions together. He agreed that he could start thinking about doing more meal preparation at home and increasing his physical activity. And now, after three months of working on those, he's coming back to us to talk about how that is going and to get more ideas from us of how to improve what's happening for him. You can see here in his journey that at month one he recognizes and shares with us that he's cooking more at home. He's doing more meal preparation and he's getting some great physical activity in. And you can see his weight's coming down a little bit. In month two he recognizes that some things in life are starting to get in the way a little bit and he's missing some of his cooking days. And by the time he comes back to us at month three he recognizes that he's re-prioritized work. Work's gotten a little more stressful and he finds himself not only prepping his meals as much and returning to some fast-food engagement but also not getting his walks in as often. His weight's still going down slightly but you can see he shared with us here that he's starting to feel frustrated. He's starting to feel like things aren't going anywhere and he's starting to do what many of our patients do which is blame themselves and feeling like he can't get it right.
Let's look at some of the factors that contribute to the development of obesity.
If we look at just a few including nutrition, physical activity and metabolism and energy expenditure we can see some common things that play a role in the development of the disease. In nutrition we know that an increased food intake affects the development of obesity, and you can see some of the things here that play into that. Emotional eating, that could be positive emotional eating, fun food, family, friends; or negative emotional eating, i.e. when I'm stressed, I eat when I'm frustrated. It could be increased food intake because we haven't had enough sleep and there are physiological drivers around that. Changes in our hunger and satiety, medications that we start with our patients that affect their hunger, all these things can play a role. Now let's think about physical activity and what contributes to physical inactivity or more sedentary behaviour in the development of obesity. Certainly, things like mobility issues, chronic fatigue, muscle, and joint pain play a very large role. It's hard to want to be active when it doesn't feel good. Other things like emotional barriers can affect whether or not we participate in physical activity. Do we feel like we can manage those physical challenges? And finally looking at metabolism and energy expenditure which may be the one we don't think of as much in terms of the development of obesity. And this reduced energy expenditure over time is affected by many things. As we age it goes down. It's different between the sexes. Genetics drive what our resting energy expenditure is and then that responds to the world in terms of epigenetics. Certainly, we see changes in fat and muscle load in different people and we can have changes that we affect in energy expenditure based on medications that we choose in patients. As we think about these factors that contribute to obesity, let's look a little more deeply into genetic abnormalities.
Genetic abnormalities that can contribute to obesity we sort of break into two areas. Monogenetic obesity, not as common and polygenic obesity, much more common. We know from various studies that the genetic role in the development of obesity is about 40 to 70% of what someone experiences in their disease. And there's a range there. But you can see here in the monogenic obesity which are typically identified very early on in age. It's typically severe obesity in early childhood. Because of the severity of the physiology, the environment doesn't play as much of a role. And these are typically single gene defects with a single mutation. There's a very high penetrance of those genes and therefore that genetic influence is large. But those are rare. More common is polygenic obesity and in this we see that is where most of our obesity lies in terms of genetic influence. This comes from hundreds of genetic variants that each have a very small effect and a low penetrance. And so, we see that environmental influence can be very high in polygenic obesity.
So, if there's a genetic underlying variable, how does that play into the metabolism and homeostasis of energy that we talked about earlier? So, let's start with the central nervous system. So, we know that obesity can result from alterations in this energy balance or homeostasis. And that starts in the hypothalamus where we believe that energy expenditure, hunger, and satiety are all regulated. And while there are many pathways, let's talk about two of the major ones, the anabolic pathway, and the catabolic pathway. You can think of the anabolic pathway as a building pathway. In that pathway from the central nervous system, it stimulates increased food intake and decreased energy expenditure because we're trying to store more energy. The catabolic pathway breaks things down. It's decreased food intake and increased energy expenditure so that we store less energy. And what we see over time is that if energy stores increase and/or decrease, they could affect things like fat stores in our body. And we know that adipose tissue sends many signals. It is not an inert substance. And here's two examples like insulin and leptin over time. And those hormonal peripheral signals send messages back to our central nervous system about this balance between weight and energy expenditure and driving things like food intake.
As we think about those central nervous system and peripheral nervous system signals, they can be influenced by a lot of outside drivers, including our macro environment, which we talked about a little earlier. That includes the built environment around physical activity, our food environment. Do we have access to the right things? For many people, it can be affected by health inequities endocrine disruptors like pollution or social cues and norms. And these macro variables have an effect on each individual in a different way, creating in that person a microenvironment that affects energetic changes. So, you can see some of the things that might be affected in the microenvironment like weight promoting medications, mood disorders, perhaps our patient does shift work and so alterations in their circadian rhythm, and of course, activity, nutrition, and their sleep. And these two together then drive that internal environment that we just talked about, that energy balance regulation that occurs in the central nervous system and contributes to driving the disease of obesity.
Well, let's come back to Roger and let's talk a little bit about how we can help him adjust his environment to support his goals. He shared some important things with us at this three-month visit. And part of what he said when he assessed what was going on for himself was, you know, sometimes I have a hard time figuring out how to prepare healthy meals or what I can cook. And what we can do is come back to him with some ideas for him to think about what fits in his life. So, try not to be so didactic or prescriptive and more open-ended about ideas that we know that are successful tools and how do those tools work for him. So, for example, okay, one option might be we could refer you to a dietician. You can consult them for some simpler recipes, develop a grocery list to make the whole process easier. You could also consider healthy grab and go options that are often available in the grocery stores now. Would either of these work for you? And open that up to discussion so he can help problem solve what happens in his life. The same thing can be done for physical activity. So, he shared with us a couple more details at that first visit and at the third visit, reminding us that he lives in a rural area. He works from home. There isn't easy access to a gym or sidewalks on the roads that he would potentially walk in. And so, he struggled by trying to find a way to be active. So, some things we might suggest include, is there another time of day when you can be active so that darkness is not available? And maybe that occurs more in your house, increasing your steps throughout the day as one of your goals. Or we could recommend simple strength exercises that he can do at home and doesn't have to be in a gym. So, really thinking about how can we individualize the care and the advice that we provide to our patients to help them strategize towards success.
One thing we think a lot about in terms of delivering obesity care is what have our patients already experienced in terms of weight bias and its impact on their journey.
Weight bias and weight stigma are real for our patients. And you can see the difference between the two here if you haven't thought about it. Weight bias involves negative attitudes and judgments towards individuals based on their weight. Weight stigma is actually a social devaluation. So perhaps using blameful language. And patients then internalize this negative weight-based sort of stereotypes or discrimination. And it can affect them very deeply. We know from research that it has many effects on both physical and mental components of our health. You can see some of those examples here. For example, weight stigma and bias can be associated with patients moving towards unhealthy eating behaviors. Or avoiding exercise, because of feeling like they can´t do it. It can be associated with psychological changes like anxiety, stress, wondering if their body image is appropriate or not and developing poor self-images around them. It can also affect disadvantages in healthcare that they experience and overall, a reduced quality of life.
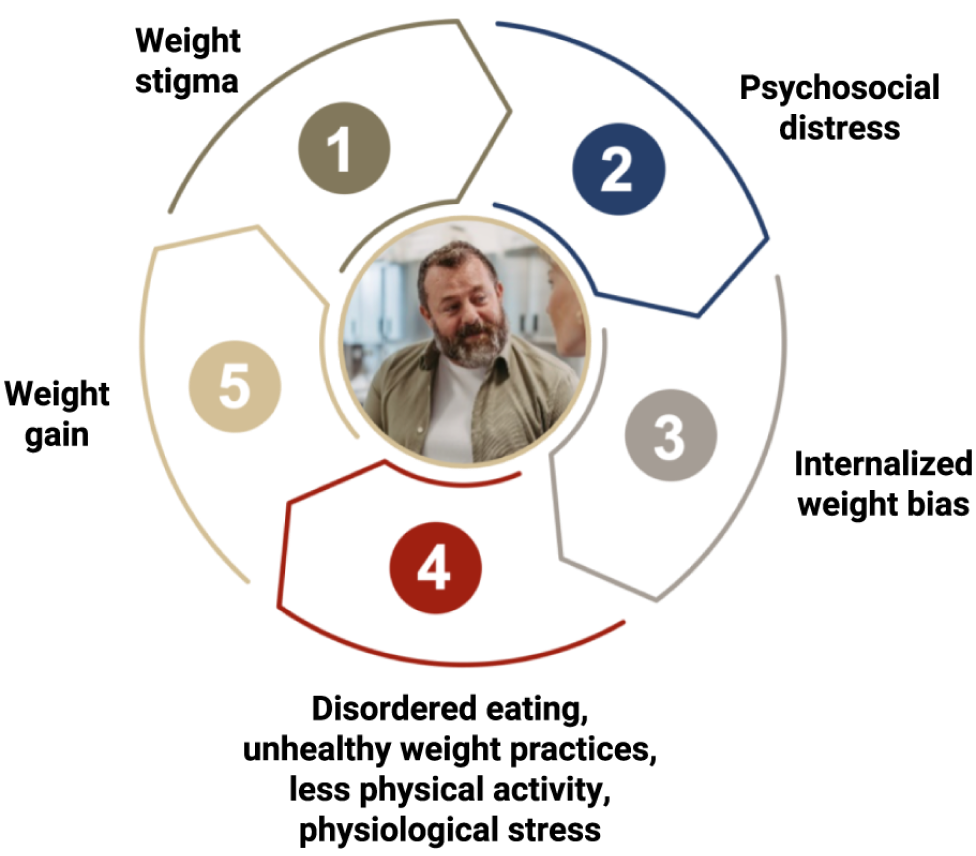
So, let's look at the negative effects of weight bias and weight stigma on individuals with obesity. It can be a vicious cycle that continues for them. And if it starts with something like weight stigma, something that was said to them, blameful language, implying their weight is their fault, it creates psychosocial distress or psychological distress in our patients. And then they internalize that weight bias even more. That can cause them to lean into unhealthy coping strategies, some of the ones that you see here, like disordered eating or unhealthy food relationships, unhealthy weight control practices, maybe minimizing their physical activity because they feel like they can't do it because they've experienced someone telling them, well, certainly you can't do that given your weight and they don't try. And physiological stress that can go along with physical activity and/or changes in their body. These stressors and internalization of weight bias lead to weight gain. And you can see now how the whole cycle starts again. Someone experiences that weight gain, they experience weight stigma or bias again, and they're going around the circle. It becomes really hard to uncouple these things.
Let's take a look at what Roger might have experienced when we think about some of the things that he shared at his first visit. So, one of the things that he shared at his first visit was that the way the weight gain started was he actually had a broken foot, which started to limit his physical activity. And he had been participating in active social engagements with his friends like biking and hiking and after gaining weight from the injury, he felt like he couldn't keep up. And then he felt like maybe they weren't inviting him anymore because of the weight gain and then he couldn't keep up. And then he started to internalize that, that he wasn't good enough to participate in these active hobbies. And so that led to him making decisions around a more sedentary lifestyle. He felt powerless. He felt like there was things that he couldn't change. He felt like if he can't be active, why is there any point in watching his diet? Because he didn't feel like it would help him lose any weight. And then we saw some of the things that we heard from him at the three month visit. He started relying on takeout meals a little bit more. He stopped doing his hiking and biking that he enjoyed so much before. And then his weight gain continued. So now you see an example of this journey that can repeat itself over and over again if we don't find a way to break that cycle.
When we think about that, think about some of the ways that weight stigma negatively impacts specific health outcomes. I think some of the most important are cardiometabolic outcomes. So, for example, we know that a patient who is experienced weight bias or stigma has a greater likelihood of having hypertension, having dysregulated cardiometabolic parameters like higher haemoglobin A1C levels, elevated C-reactive protein levels, changes in their cortisol. It also, as we saw, can increase the risk of more weight gain. And then things that maybe aren't as obvious to us. So, changes in our patient's mental health, anxiety, stress, changes in their eating behaviour, which we want them to continue to report to us so that we can help them and encourage them to make great choices, and changes in their physical activity that we already saw with Roger. So, there are many negative impactive health outcomes that can happen secondary to weight bias, stigma, and weight discrimination.
But there are things that we can do to make improvements in how our patients experience time in our clinic. Because remember, we started by thinking about what is the role that we can play to improve the obesity care that our patients experience. So, let's talk about some of the strategies. And what I'd love for you to do is think about in the items that I mentioned, where do you see opportunities in your health care environment to improve what your individuals living with obesity, struggling with obesity, that come to you for care experience?
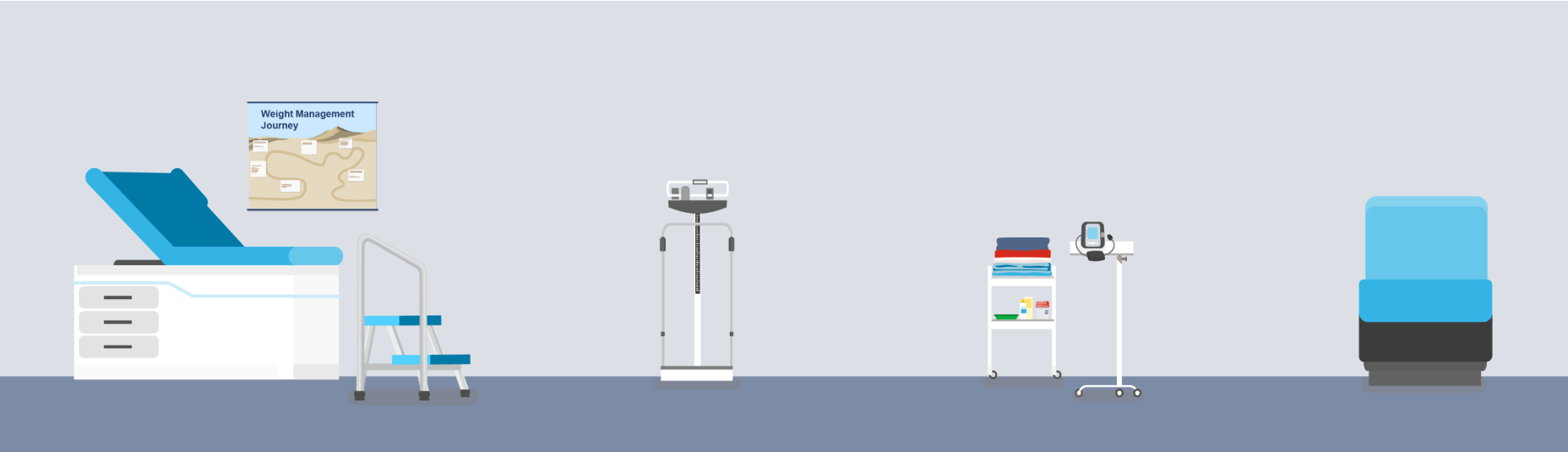
So, let's start even before our patient gets to us, even before they sit down in the waiting room. Have we made the clinic open and accessible to our patients? Do the restrooms have grab bars and split lavatory seats to allow for getting up and down off the facilities and using them in a hygienic way? Are we providing weight sensitive reading materials? This is very interesting. We can take some typical magazines that we might have in any other doctor's office. And yet when we look at the covers, it talks about Hollywood diets or fad diets or extremes of physical activity or maybe unhealthy approaches to body image. And so, making sure that we have great weight sensitive reading material. Is there enough room for people in our clinics? Is there enough space between the chairs? And do those places to sit, are they welcoming to a patient? Are they open arm? Do they have firm surfaces so our patients can more easily get up and down out of those chairs? All the things for us to consider. Now let's move to, I think, something that's really important when patients come to see us about getting care around obesity. And that is the scale. Is that scale in a place that provides privacy and confidentiality for your patients? Because it can be a very sensitive experience. Is it accessible to individuals with disabilities? Can someone with a wheelchair roll on and off of the scale? Are there handles or supports so the patient can utilize the scale? And does the scale have an appropriate wide base and an appropriate accessibility from a top weight standpoint? I think one of the most traumatic things that can happen to a patient is to step on a scale and realize the scale can't measure their weight. So being sensitive about that and having the right equipment. Let's think about other things in our exam room. Do we have wide examination tables that will facilitate an appropriate interaction with our patients? Is there a step stool with a handle to examine that table access? Pulling out that little step that we often have the bottom of our exam tables and then asking someone with obesity to face forward and turn around on that small step can be very daunting. Partly because balance can be an issue for them. Do we have the right equipment to provide sensitivity to our patients? Are we providing large enough gowns for them during examinations? Do we provide equipment that allows them to do the tests that we want them to do? And finally, are we using good equipment ourselves? Are we using the appropriate blood pressure cuffs? Most patients struggling with obesity either need a large size adult cuff or a thigh cuff to get an appropriate blood pressure reading. And if we use the wrong size cuff, we get elevated readings if the cuff is too small and those are artificially elevated. Again, just like the exam room, can we provide sturdy armless chairs just like we did in the waiting room? And then thinking about the messaging that we deliver, the interactions that our staff have with our patients, and we have. Are we providing non-judgmental information and commentary that's private and recognizes the sensitivity of the subject? Are we asking individuals for permission to be weighed at each visit? And do we emphasize goals beyond the scale? So not just the number on the scale, but how are they feeling? How are they moving? What goals in their life are they now able to achieve? Are there other health markers like those cardiometabolic parameters that we mentioned that can be leverage points to demonstrate improvement for our patients as they succeed? All of these things become really important when we're trying to create an environment that is conducive to providing great care, excellent care for individuals living with obesity.
When you think about your practice, which areas of your office do you think you could improve to mitigate weight bias? We gave a lot of examples just now and you might have thought, wow, that's something I could do tomorrow. So, think about things that you might change in that way.
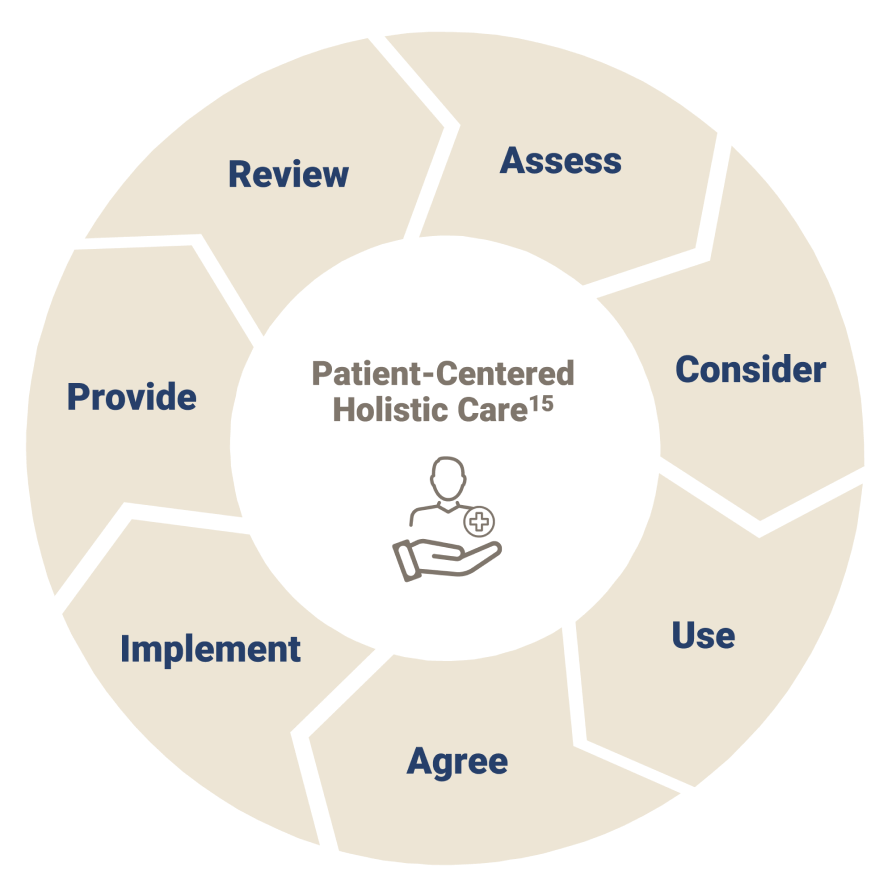
As we look broadly on the contributing factors to obesity that can impact how we collaborate with our patients, here's sort of a nice overview of how we can deliver patient-centred holistic care. Remember, we want to ask permission first to talk about their weight and assess how the patient is doing in terms of the disease. Consider the factors that might affect their treatment choices, so weight-related complications, social determinants of health, access to treatments. And then in our communication with patients, as we saw with Roger, trying to be open-ended and use motivational interviewing to help the patient come to the solutions that work in their life, and then agreeing together on those solutions and helping our patients implement those solutions. That means we have to provide resources for them. Maybe we don't have a dietician in our clinic, but we provide the community resource for that. Patients might also not realize what opportunities they might have in their community to be physically active or to experience emotional support. So, making sure that we provide that ongoing support and monitoring so that we can minimize the barriers or the burdens that get in their way.
As we come back to where we started, this comprehensive view of obesity,
I want to bring us back to the four pillars that we mentioned before, psychological, lifestyle/behavioural, environmental, and social and biological factors. And let's bring this back one more time to our patient Roger and sort of remember
the things that he shared. From a psychological standpoint, he shared that he had internalized some of this weight bias that he maybe misunderstood by not participating in activity with his friends, that he was experiencing increased stress from work that was getting in the way of him participating in nutrition planning like he wanted to. That working from home and stress around that was leading to more frequent eating out, which was different than the plan that he'd started. So how do we move him into a place where he can manage that better? And then some of the environmental things. So, remember, he's lost contact with some of his more active friends. How do we encourage him to reengage with that? What about helping him get access to mental health support if he needs it or dietary education if he needs it? And then thinking about those biological factors, because remember, they are underlying all of this. It starts with genetic and biology. So, helping remember that genetics is part of what plays into what he experiences from a disease state or any of our patients, and that changes in metabolism and hormones make treating obesity more challenging and recognizing that helps our patients understand that it's not their fault, it's their physiology.
If we come back to what we can do to create an effective weight management plan with our patients, here are some ideas. So, remember to assess obesity-related complications because we can treat more than one disease at once. Whether each individual patient's values, their support system, their lifestyle, we've got to dig in and learn about that to meet them where they are and help them make the choices that work best for them. That collaborative approach, and we all know how to set smart goals with patients and bringing it back to that so that the goals they set are attainable. And then finally providing that support they need. And one thing we haven't talked about, which is really thinking about what is the patient's readiness for change. When we met Roger at the three-month visit, he was coming back to share with us how things were going, so he was already in action. Some of our patients may come to us in contemplation, preparation, pre-contemplation, and where we meet them and the conversations we have with them have to be driven a little by that.
And I just want to summarize by challenging you to maybe take one action in your clinic tomorrow or next week to think about how you can improve your practice for your patients living with obesity. Some ideas might be change one thing that we talked about together. Perhaps you want to evaluate your clinical space and decide which things could be easily adjusted. Thinking about doing staff training so they know how to deliver sensitive and careful information to patients that doesn't move into weight bias and weight stigma. And finally, identifying resources that you can provide for your patients that continue to help them beyond the visit that they sit in with you in the practice. I just want to thank you for sharing your time today. I want to encourage you to think about the ways that we can all improve the role that we have in obesity care. And finally, just remember, treat early, treat always, treat obesity.