Comprehensive Obesity Care
Importance of Diagnosis
Obesity is a complex, multifactorial disease.1 Diagnosing obesity can be a critical first step in weight management and health outcomes for patients.
How can your patients benefit from obesity diagnosis and comprehensive care? Obesity is a complex multifactorial disease that requires comprehensive care to address the multisystem complications it is associated with, such as, osteoarthritis, hypertension and depression. Early diagnosis of obesity may lead to improvements in weight and obesity-related complications. New communication and care approaches, like the diagnostic term adiposity-based chronic disease, may help address barriers to diagnosis and improve patient outcomes. If you are interested in learning more about the benefits of obesity diagnosis and comprehensive care, follow the link on the screen.
Obesity as a disease
“Obesity is a chronic, progressive, relapsing, and treatable multifactorial neurobehavioral disease, wherein an increase in body fat promotes adipose tissue dysfunction and abnormal fat mass physical forces, resulting in adverse metabolic, biomechanical, and psychosocial health consequences.”
– The Obesity Medicine Association1
In 2016 2:
- 650 million people ≥18 years of age had obesity
- >340 million people 5-19 years of age had obesity or overweight
Image adapted from Our World in Data.3
Obesity is not simply a “comorbidity” or “risk factor” for other conditions1,4-6:
- Can be caused by a multitude of genetic and environmental factors outside food choice
- Shares many of the same pathogenic processes as aging
- Is a major cause of cardiovascular disease (CVD), cancer, sleep apnea, type 2 diabetes, and other related metabolic conditions4-6
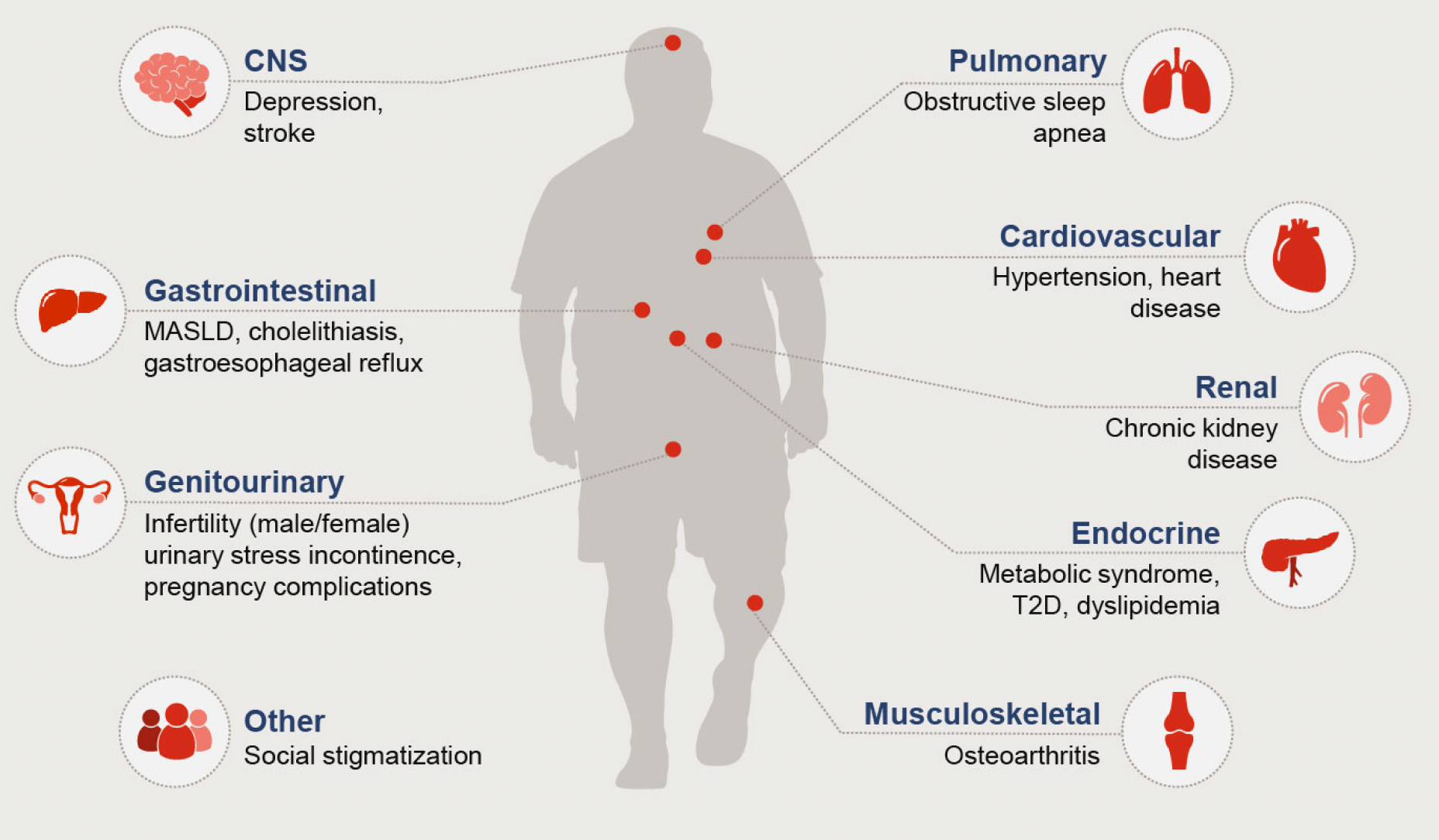
Cancer
Colorectal, postmenopausal, breast, endometrial, gastrointestinal, liver
Cardiovascular
Hypertension, heart disease
Central Nervous System (CNS)
Depression, stroke
Endocrine
Metabolic syndrome, type 2 diabetes, dyslipidemia
Gastrointestinal
Metabolic dysfunction-associated steatotic liver disease (MASLD), cholelithiasis, gastroesophageal reflux
Genitourinary
Infertility (male/female), urinary stress incontinence, pregnancy complications
Infections
Sensitivity to influenza and COVID-19
Musculoskeletal
Osteoarthritis
Pulmonary
Obstructive sleep apnea
Renal
Chronic kidney disease
Other
Social stigmatization
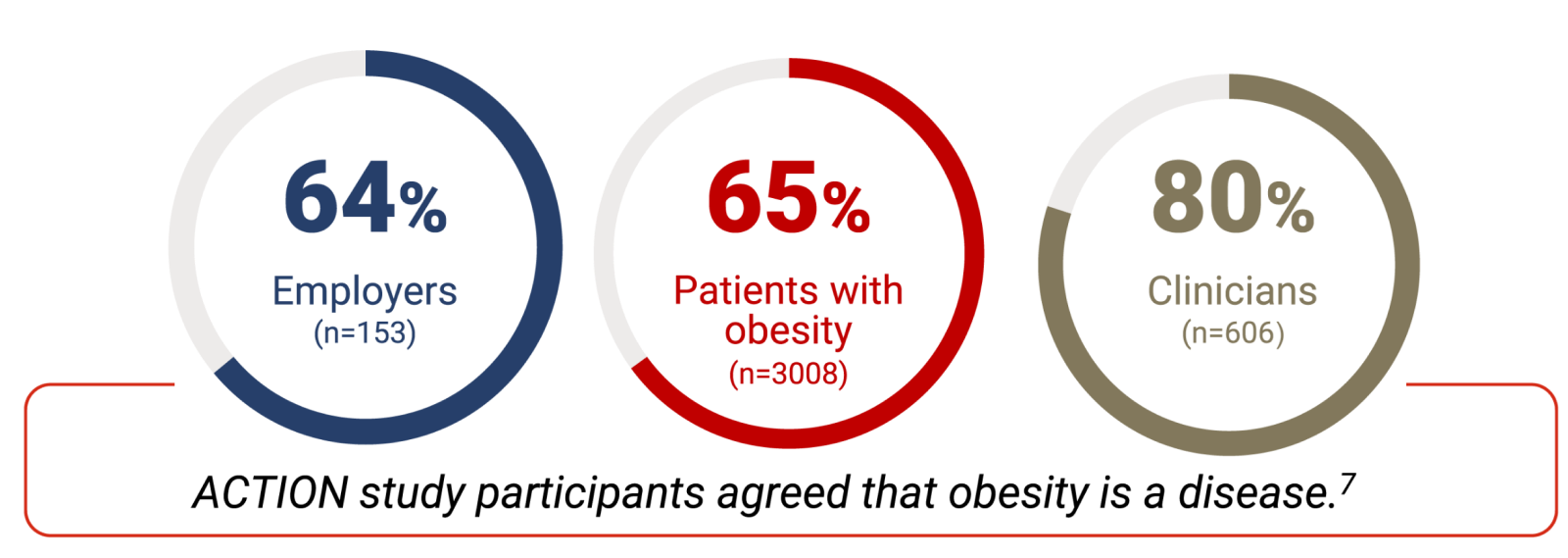
- 64% of employers (n=153)
- 65% of patients with obesity (n=3008)
- 80% of clinicians (n=606)
Action study participants agreed that obesity is a disease.7
Screening and Diagnosing Criteria for Obesity
The diagnosis of obesity can be made through the clinical interpretation of body mass index (BMI), taking into consideration other indicators of adiposity, as well as the presence of obesity-related complications 8,9
- Overweight: ≥25.0 to <30.0
- Class 1 obesity: ≥30.0 to <35.0
- Class 2 obesity: ≥35.0 to <40.0
- Class 3 obesity: ≥40.0
- Waist circumference11
- Waist-to-height ratio11
- Waist-to-hip ratio11
- Body composition technologies (eg, bioelectrical impedance analysis)8
- BMI and other indicators of obesity, such as waist circumference
- Individual differences in body composition (eg, lean mass vs fat mass)
- Associated with age, sex, ethnicity, and physical activity
- Presence of adiposity-related complications
- Weight management journey
- Individualized goals
- BMI10
- American Association of Clinical Endocrinology (AACE)/American College of Endocrinology (ACE) stages of obesity8
- Edmonton Obesity Severity Scale9
Roger, a hypothetical patient, is visiting his clinician for an annual physical examination.
Roger has a history of weight gain after a foot fracture and experiences frustration and embarrassment at his inability to keep up with his previous physically active hobbies such as hiking and biking.
In the past 2 years, Roger lost weight using a commercial diet plan but regained the weight when he could no longer afford the diet meals.

- Age: 57
- Weight: 207 lb
- Height: 5 ft 5 in
- BMI: 34.5 kg/m2
- Waist circumference: 43 in
Roger’s clinician will clinically ASSESS him to determine whether a diagnosis of obesity is appropriate. Based on this diagnosis and his obesity stage, she can better ADVISE him of treatment goals and options.

Diagnosing and Treating Patients With Obesity
Early Diagnosis of Obesity May Lead to Improvements in Weight and Other Clinical Outcomes1,12

Weight loss of 2%-5% results in improvements in glycemic measures and triglyceride levels1,12
Weight loss of 5%-10% improves mobility, high-density lipoprotein (HDL) levels, urinary incontinence, and sexual function and reduces healthcare costs1,12
Weight loss of 10%-15% or more can improve steatohepatitis and sleep apnea1,12
(OR = 1.3; CI: 1.2-1.3)13
(OR = 1.4; CI: 1.3-1.4)13
Learn more about comprehensive obesity care.
Includes how to discuss obesity with patients and Roger’s weight loss journey.
References
- Bays H, Golden A, Tondt J. Thirty obesity myths, misunderstandings, and/or oversimplifications: an Obesity Medicine Association (OMA) clinical practice statement (CPS) 2022. Obesity Pillars. 2022;3:100034.
- World Health Organisation. Obesity and overweight. World Health Organisation. Accessed October 26, 2023. https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight
- Ritchie H, Roser M. Obesity. Our World in Data. Accessed October 26, 2023.https://ourworldindata.org/obesity#
- Tsai AG, Bessesen DH. Obesity.Ann Intern Med. 2019;170(5):ITC33-ITC48. doi:10.7326/AITC201903050
- Sarma S, Sockalingam S, Dash S. Obesity as a multisystem disease: trends in obesity rates and obesity-related complications. Diabetes Obes Metab. 2021;23(suppl 1):3-16.
- Chan W-K, Chuah K-H, Rajaram RB, Lim L-L, Ratnasingam J, Vethakkan SR. Metabolic dysfunction-associated steatotic liver disease (MASLD): a state-of-the-art review. J Obes Metab Syndr. 2023;32(3):197-213.
- Kaplan LM, Golden A, Jinnett K, et al. Perceptions of barriers to effective obesity care: results from the National ACTION Study. Obesity (Silver Spring). 2018;26(1):61-69.
- Garvey WT, Mechanick JI, Brett EM, et al. American Association of Clinical Endocrinologists and American College of Endocrinology comprehensive clinical practice guidelines for medical care of patients with obesity. Endocr Pract. 2016;22(7):842-884.
- Rueda-Clausen CF, Poddar M, Lear SA, Poirier P, Sharma AM. Canadian adult obesity clinical practice guidelines: assessment of people living with obesity. Obesity Canada. Accessed May 29, 2023.https://obesitycanada.ca/guidelines/assessment
- Defining adult overweight & obesity. Centers for Disease Control and Prevention. Accessed November 7, 2023.https://www.cdc.gov/obesity/basics/adult-defining.html
- Bray GA, Heisel WE, Afshin A, et al. The science of obesity management: an Endocrine Society scientific statement. Endocr Rev. 2018;39(2):79-132.
- Ryan DH, Yockey SR. Weight loss and improvement in comorbidity: differences at 5%, 10%, 15%, and over. Curr Obes Rep. 2017;6(2):187-194.
- Ciemins EL, Joshi V, Cuddeback JK, et al. Diagnosing obesity as a first step to weight loss: an observational study. Obesity.2020;28(12):2305-2309.
VV-MED-156376
Please rate your satisfaction with the content on the following statements:
Very Dissatisfied
Dissatisfied
Neutral
Satisfied
Very Satisfied