Chronic Lymphocytic Leukemia (CLL)
Aspects of Supportive Care
CLL management and supportive care involve shared decision making between the patient and the medical team to ensure the following:
Deciding on a treatment plan that matches patient needs and goals1,2
Patient staying up to date with vaccinations3
Proactive infection prevention through mask wearing and frequent handwashing4
Regular primary care provider visits, dermatologic screening, and other cancer screening5-8
Support system for patients with CLL9-11
CLL is a lifelong diagnosis, and patients benefit from strong social support
Medical care team
- Orchestrate care
- Provide educational resources
Mental health
Treat emotional toll of disease
Social worker
Help identify support
Patient support groups
- Solidarity through similar experiences
- Patient education
Caregiver
- Attend patient visits
- Partner with patient at home
Adverse Event Management
Common adverse events associated with CLL treatments
Each CLL therapy has a unique adverse event profile; however, certain adverse events are common to many treatment types and require timely clinical management and/or prophylaxis
Infection
(13%-81%)12-22,aDyspnea
(9%-28%)18,20,21,23,bAnemia
(5%-67%)12,14-16,19-27,aDiarrhea
(14%-51%)12-25,27,aThrombocytopenia
(6%-24%)12,16,19-28,aFatigue
(5%-36%)13-15,18-28,aArthralgia
(6%-26%)13-16,23,28,cHeadache
(2%-38%)13,15,18,22,23,25,28,aInfection prevention in patients with CLL
The 5-year risk for severe infections in CLL is 26%29
Recommended vaccinations for patients with CLL30,a
- Recombinant hepatitis B
- COVID-19 vaccine
- Pneumococcal vaccine
- Seasonal influenza vaccine
- Recombinant zoster vaccine
Strategies for infection prevention in patients with CLL
The 5-year risk for severe infections in CLL is 26%29
Bacterial infections30
- No routine antibiotic prophylaxis
- Ig replacement therapy for severe hypogammaglobulinemia and/or recurrent or severe infection
- Monitor ANC
Fungal infections30
- Consider prophylaxis
- In frail older patients with R/R CLL and/or prolonged neutropenia
- Those with previous fungal infections
- Patients receiving chronic, concomitant steroids
Viral infections30
- Monitor for infection/pretreatment of HBV, HCB, HIV, HSV 1/2, VZV, and CMV prior to starting CLL therapy
- If HBV reactivation detected, preemptive therapy with antivirals
The 5-year risk for severe infections in CLL is 26%29
Standardized incidence ratiosa for second primary cancers after CLL31
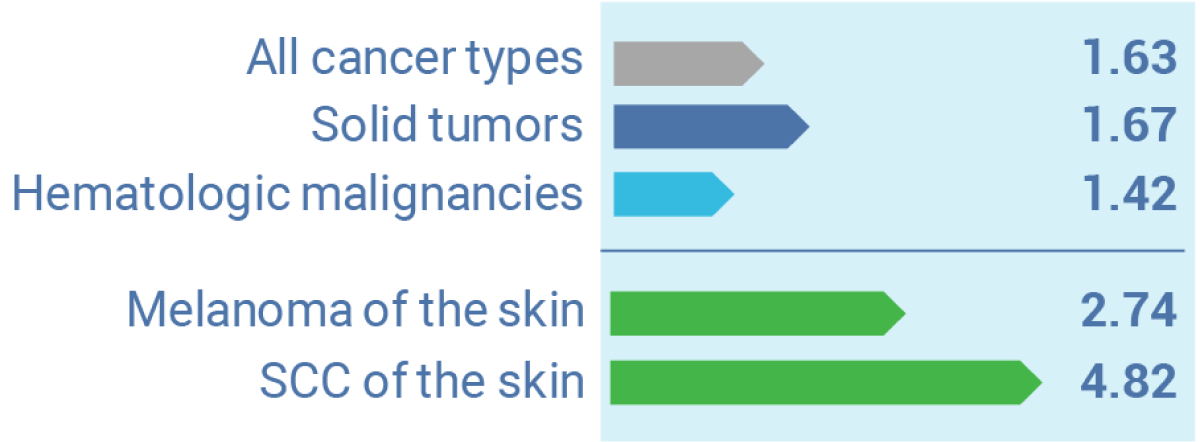
The graph illustrates incidence ratios of secondary primary malignancies in patients with CLL of 1.63 for all cancer types, 1.67 for solid tumors, 1.42 for hematologic malignancies, 2.74 for melanoma of the skin, and 4.82 for squamous cell carcinoma of the skin.
aStandard incidence ratio is a ratio of the number of cancers observed in a given population compared with the number expected.
An increased risk of secondary primary malignancies in patients with CLL necessitates timely cancer screening5,31
Annual dermatologic skin screening is recommended for skin cancer prevention5
Cancer screening guidelines should be followed closely for breast, cervical, colon, prostate cancers, and lung cancer for smokers6
Composition of the multidisciplinary team in the care of patients with CLL
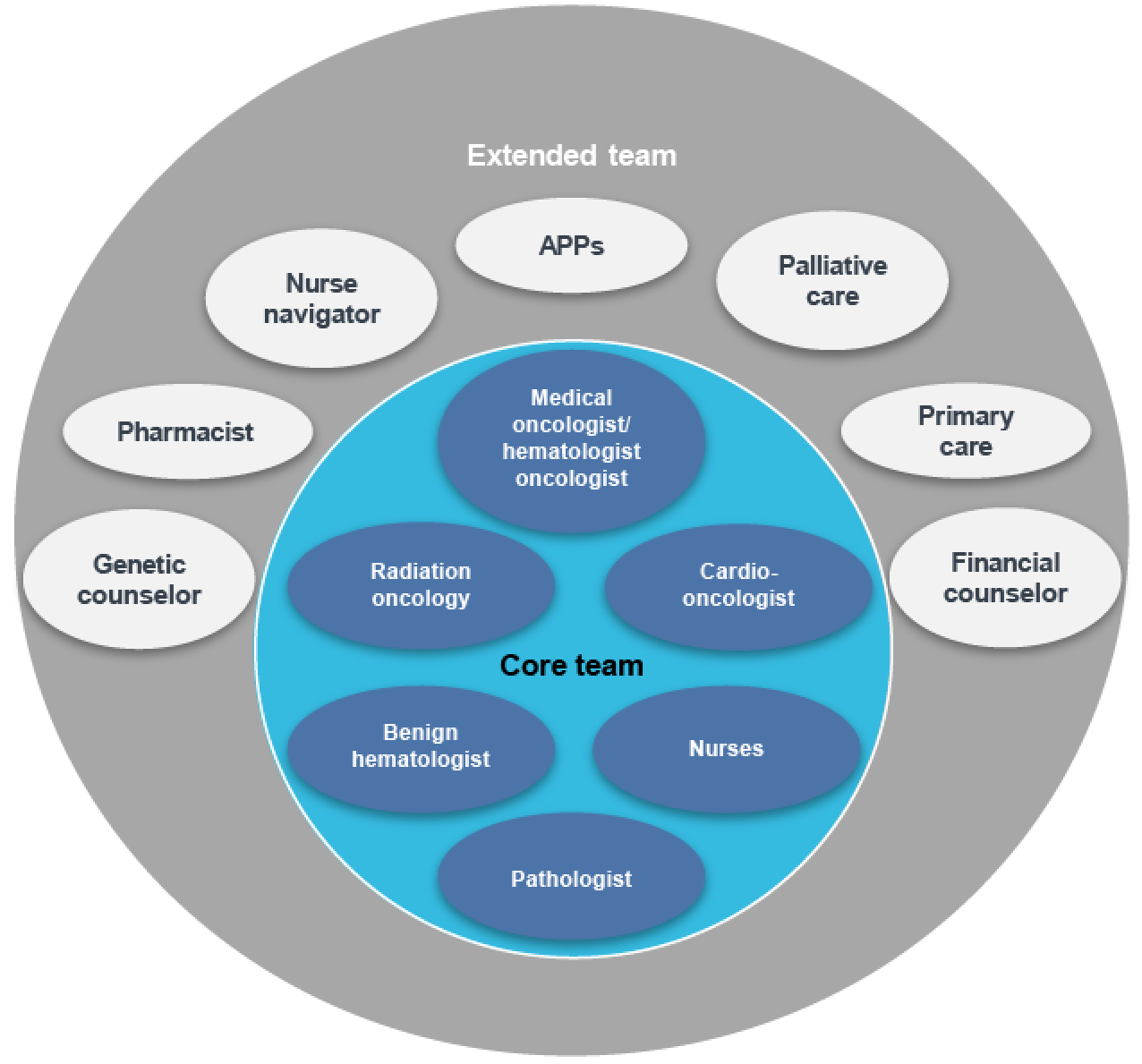
Multidisciplinary care involves cooperation between different specialties in order to improve patient care, and has become a major focus of contemporary cancer management32,33
A multidisciplinary care team in oncology can include34
- Core team: participates in tumor board meetings and primary decision-making and usually consists of medical oncologist/hematologist, radiation oncology, benign hematologist, pathologist, nurses, and cardiologist
- Extended team: participates in management of patient care and social services. It can include genetic counselor, pharmacist, nurse navigator, APPs, palliative care, primary care, and financial counselors
References
- Katz SJ, et al. J Oncol Pract. 2014;10(3):206-208.
- Brown R, et al. J Clin Oncol. 2012;30(8):857-862.
- CLL Society. Accessed August 12, 2024. https://cllsociety.org/2022/03/vaccinations-for-patients-with-cll-sll
- LLS. Infections. Accessed August 12, 2024. https://www.lls.org/treatment/managing-side-effects/infections
- Mansfield AS, et al. J Oncol Pract. 2014;10(1):e1-e4.
- Welch A. Recognizing secondary malignancies in CLL. Accessed May 8, 2024. https://www.onclive.com/view/recognizing-secondary-malignancies-in-cll
- Schneider MA. When a cure isn’t an option. Accessed August 12, 2024. https://ashpublications.org/ashclinicalnews/news/7672/When-a-Cure-Isn-t-an-Option
- HealthTree Foundation for CLL. Infection prevention for CLL patients with Dr. Meghan Thompson. Accessed August 12, 2024. https://healthtree.org/cll/community/articles/cll-infection-prevention-dr-meghan-thompson
- Bell R. J Adv Pract Oncol. 2017;8(5):462-473.
- Frankly Speaking About Cancer. Accessed August 12, 2024. https://www.cancersupportcommunity.org/sites/default/files/fsac/CLL_Improving_Communication_with_Your_Patients.pdf
- Academy of Oncology Nurse & Patient Navigators. Navigating chronic lymphocytic leukemia: the critical importance of the first 90 Days. Accessed August 12,2024. https://aonnonline.org/navigation-tools/4879:navigating-chronic-lymphocytic-leukemia-the-critical-importance-of-the-first-90-days
- Eichhorst B, et al. N Engl J Med. 2023;388:1739-1754.
- Sharman JP, et al. Leukemia. 2022;36:1171-1175.
- Barr PM, et al. Blood Adv. 2022;6:3440-3450.
- Tam CS, et al. Lancet Oncol. 2022;23:1031-1043.
- Brown JR, et al. N Engl J Med. 2023;388:319-332.
- Brown JR, et al. [abstract]. Blood. 2023;142 :Abstract 202.
- Mato AR, et al. N Engl J Med. 2023;389:33-44.
- Stilgenbauer S, et al. J Clin Oncol. 2018;36:1973-1980.
- Kabadi SM, et al. Cancer Med. 2019;9:3803-3810.
- Furman RR, et al. N Engl J Med. 2014;370:997-1007.
- Siddiqi T, et al. Lancet. 2023;402(10402):641-654.
- Byrd JC, et al. J Clin Oncol. 2021;39:3441-3452.
- Flinn IW, et al. Blood. 2018;132:2446-2455.
- Gopal AK, et al. N Engl J Med. 2014;370:1008-1018.
- Fischer K, et al. N Engl J Med. 2019;380(23):2225-2236.
- Seymour JF, et al. N Engl J Med. 2018;378:1107-1120.
- Patel H, et al. Expert Rev Pharmacoecon Outcomes Res. 2023;23:651-658.
- Grywalska E, et al. Cells. 2020;9(11):2398.
- Rivera D, Ferrajoli A. Curr Oncol Rep. 2022;24(8):1003-1014.
- van der Straten L, et al. Blood Cancer J. 2023;13(1):15.
- Goede V, Stauder R. J Geriatr Oncol. 2019;10:497-503.
- Taberna M, et al. Front Oncol. 2020;10:85.
- Berardi R, et al. Cancer Manag Res. 2020;12:9663-9374.
- Selby P, et al. Am Soc Clin Oncol Educ Book. 2019;39:332-340.
- Tariman J. ASH Clinical News. 2016. Welcome to the era of shared decision-making. Accessed August 12, 2024. https://ashpublications.org/ashclinicalnews/news/2559/Welcome-to-the-Era-of-Shared-Decision-Making
- Association of Community Cancer Centers. Multidisciplinary chronic lymphocytic leukemia care. Accessed August 12, 2024. https://www.accc-cancer.org/docs/projects/chronic-lymphocytic-leukemia-(cll)/cll-models-of-effective-care-delivery.pdf?sfvrsn=3ebbf592_2
VV-MED-163244
Please rate your satisfaction with the content on the following statements:
Very Dissatisfied
Dissatisfied
Neutral
Satisfied
Very Satisfied