Chronic Lymphocytic Leukemia (CLL)
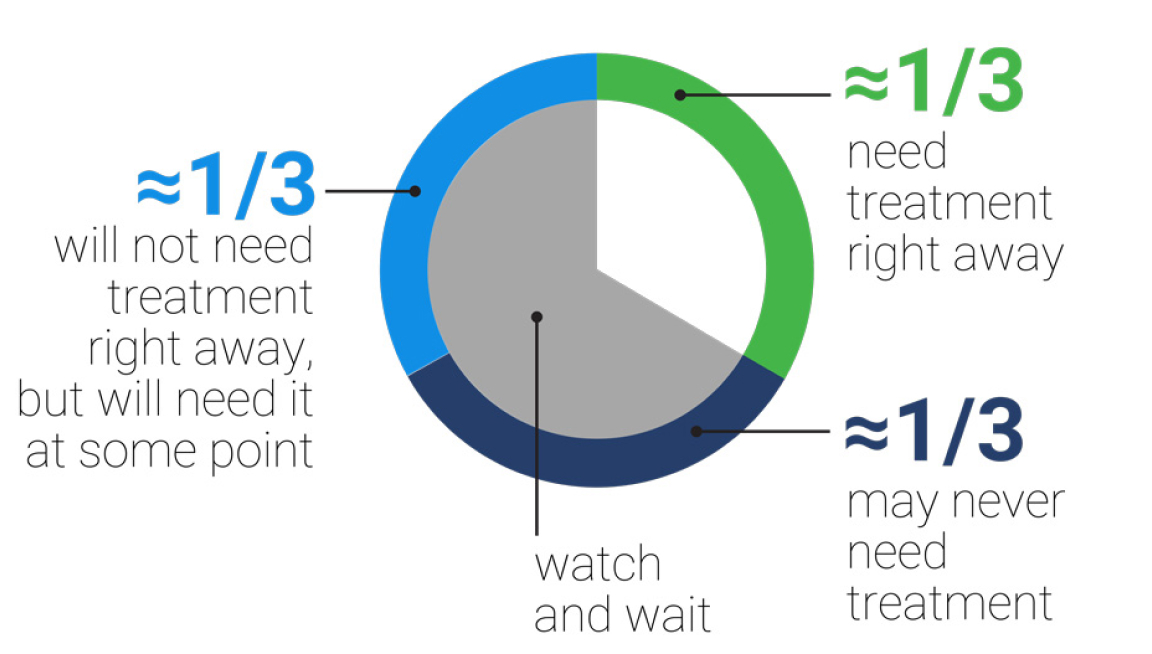
Graph showing an approximate proportion of patients with CLL who need treatment right away (≈1/3), those who will not need treatment right away but will need it at some point (≈1/3), and patients with CLL that may never need treatment (≈1/3). Overall, ≈2/3 of patients are placed in the “watch and wait” category.
When do patients with CLL need treatment?
iwCLL indications for treatment3,a
Lymph nodes
Massive (ie, ≥10 cm), progressive, or symptomaticLiver and/or spleen size Massive
(ie, ≥6 cm below the left costal margin), progressive, or symptomaticConstitutional symptom
Disease-related symptomsbCirculating lymphocyte count
Progressive ≥50% over a 2-month period, or lymphocyte doubling time <6 monthscPlatelet count
Worsening thrombocytopenia <100 x 109/L due to progressive marrow failuredHemoglobin
Worsening anemia <10 g/dL due to progressive marrow failuredBone marrow
Progressive marrow failure as per aboveExtranodal
Symptomatic or functional extranodal involvement (eg, skin, kidney, lung, spine)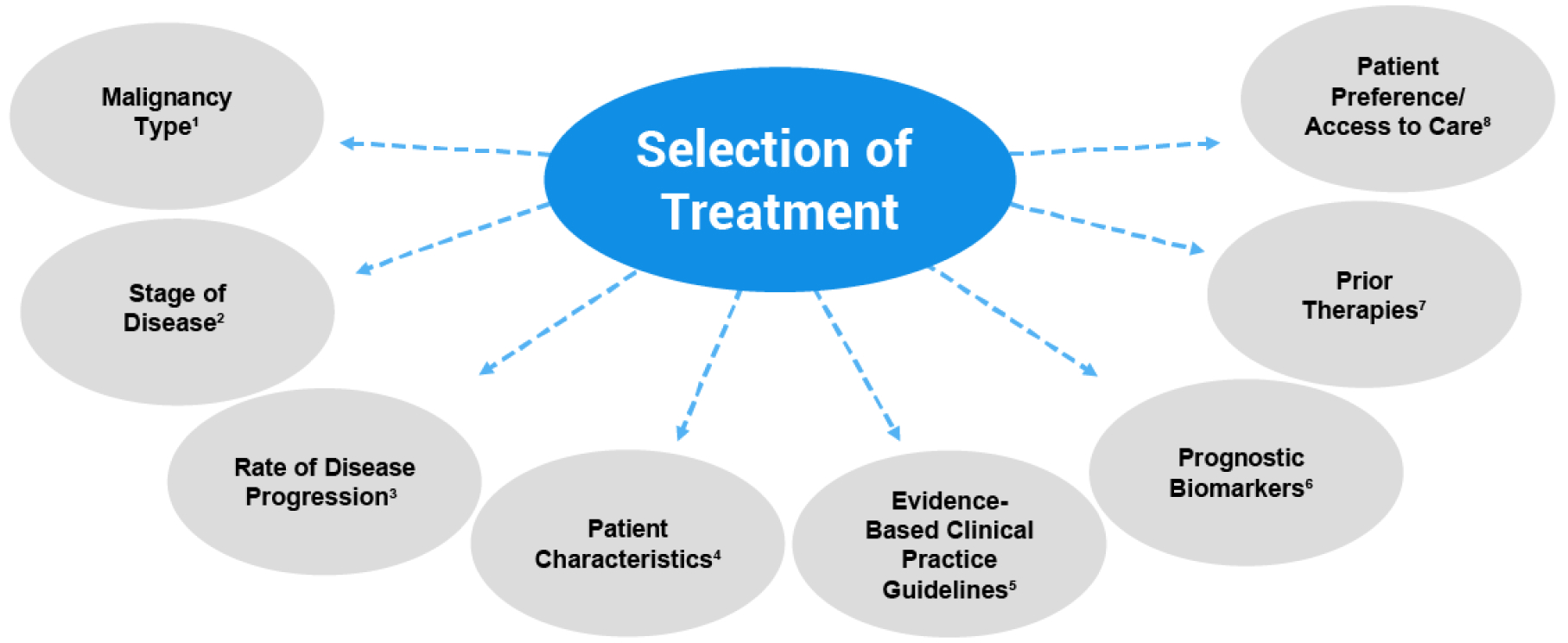
Selection of treatment in CLL depends on malignancy type, stage of disease, rate of disease progression, patient characteristics, evidence-based clinical practice guidelines, prognostic biomarkers, prior therapies, patient preference/access to care
- Developing a treatment plan for patients with CLL involves shared decision-making between patients and providers after considering stage of disease, risk of progression, overall prognosis, and potential side effects12,14
- For patients with CLL in which treatment is indicated, the presence or absence of del(17p) and TP53 mutations are most often used to direct treatment selection13
Leverage SHARE principles for shared decision making14,16
Shared patient decision making occurs when HCP and patient work together to make a healthcare decision that is in the best interest of the patient

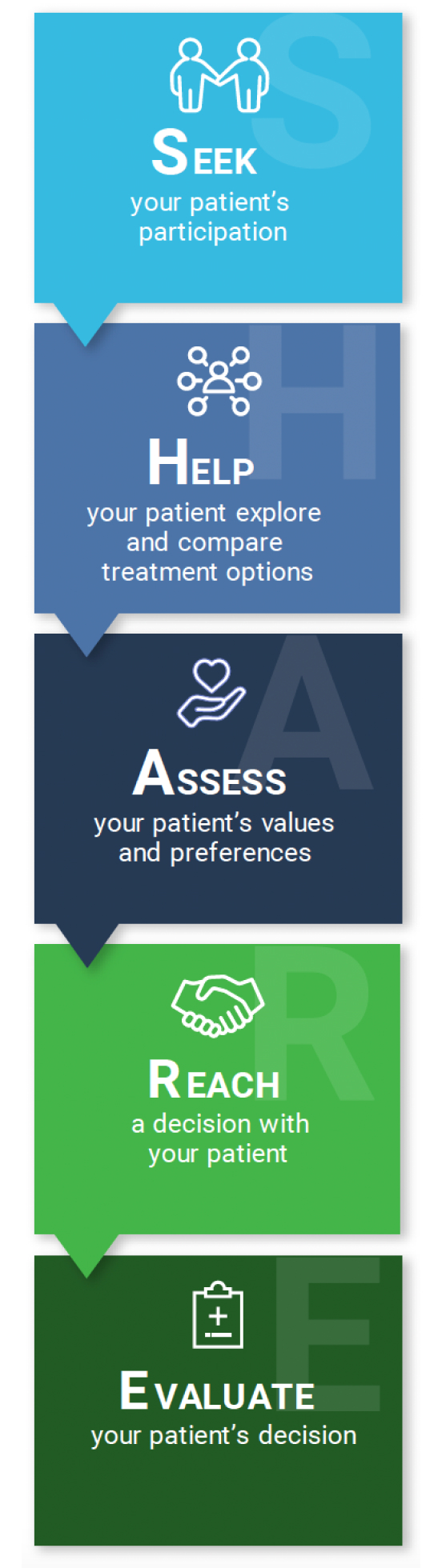
To use share principles for shared decision making, seek your patient’s participation, help your patient explore and compare treatment options, assess your patient’s values and preferences, reach a decision with your patient, and lastly, evaluate your patient’s decision
References
- Shadman M. JAMA. 2023;329(11):918-932.
- HealthTree Foundation for Chronic Lymphocytic Leukemia. What is watch and wait for CLL? Accessed August 12, 2024. https://healthtree.org/cll/community/articles/what-is-watch-and-wait-for-cll
- Hampel PJ, Parikh SA. [published correction appears in Blood Cancer J. 2022;12(12):172]. Blood Cancer J. 2022;12(11):161.
- Jamil A, Mukkamalla SKR. Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560826/
- Cheson BD, et al. J Clin Oncol. 2014;32(27):3059-3068.
- Lumish M, et al. J Hematol Oncol. 2021;14(1):5.
- Terret C, et al. Expert Rev Hematol. 2015;8(3):329-341.
- . InformedHealth.org [Internet]. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG); 2006-. In brief: What are clinical practice guidelines? [Updated 2016 Sep 8]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK390308/
- Sun R, et al. Mod Pathol. 2016;29(10):1118-1142.
- Ngu H, et al. Am Soc Clin Oncol Educ Book. 2022;42:1-14.
- Loh KP, et al. Blood Adv. 2020;4(21):5492-5500.
- Lymphoma Action. CLL and SLL. Accessed August 12, 2024. https://lymphoma-action.org.uk/types-lymphoma/chronic-lymphocytic-leukaemia-cll-and-small-lymphocytic-lymphoma-sll#what-is
- Campo E, et al. Haematologica. 2018;103(12):1956-1968
- Katz SJ, et al. J Oncol Pract. 2014;10(3):206-208.
- LUNGevity Transforming Lung Cancer. Shared decision-making. Accessed May 12, 2024. https://www.lungevity.org/research/patient-focused-research-center-patient-force/shared-decision-making
- Agency for Healthcare Research and Quality. The SHARE approach: a model for shared decision making. Accessed May 12, 2024.https://www.ahrq.gov/sites/default/files/publications/files/share-approach_factsheet.pdf
VV-MED-163244
Please rate your satisfaction with the content on the following statements:
Very Dissatisfied
Dissatisfied
Neutral
Satisfied
Very Satisfied